How to use this page
This journey covers the digestive system from mouth to anus, in six stops spread across one week. Each stop takes about 25–30 minutes and follows the same rhythm:
- A little reading to set the scene.
- A little interaction (H5P activities embedded in your course page; click-to-reveal labeling here).
- A little confirmation — a mini self-check with feedback.
One topic per day:
- Stop 1 — Mon. Mouth & esophagus. The two stratified-squamous regions of the gut.
- Stop 2 — Tue. Stomach. Pits, glands, parietal vs. chief cells.
- Stop 3 — Wed. Small intestine. Villi + Brunner's vs. Peyer's.
- Stop 4 — Thu. Large intestine, rectum, anus. Flat surface, deep crypts, taenia coli.
- Stop 5 — Fri. Accessory glands. Salivary, pancreas, liver, gallbladder.
- Stop 6 — BONUS. Immune structures. Tonsils, MALT, Peyer's patches, appendix.
Click any stop to expand. Progress is saved automatically in this browser.
Big-picture preview
Before diving into the six stops, take five minutes to map the whole tract — every organ from mouth to anus, plus the four accessory glands. The activity below is the reference picture for the rest of the week.
1 Mouth & Esophagus Day 1 (Mon) • ~30 min • Where digestion begins; the two stratified-squamous regions of the gut ✓
The work of the mouth
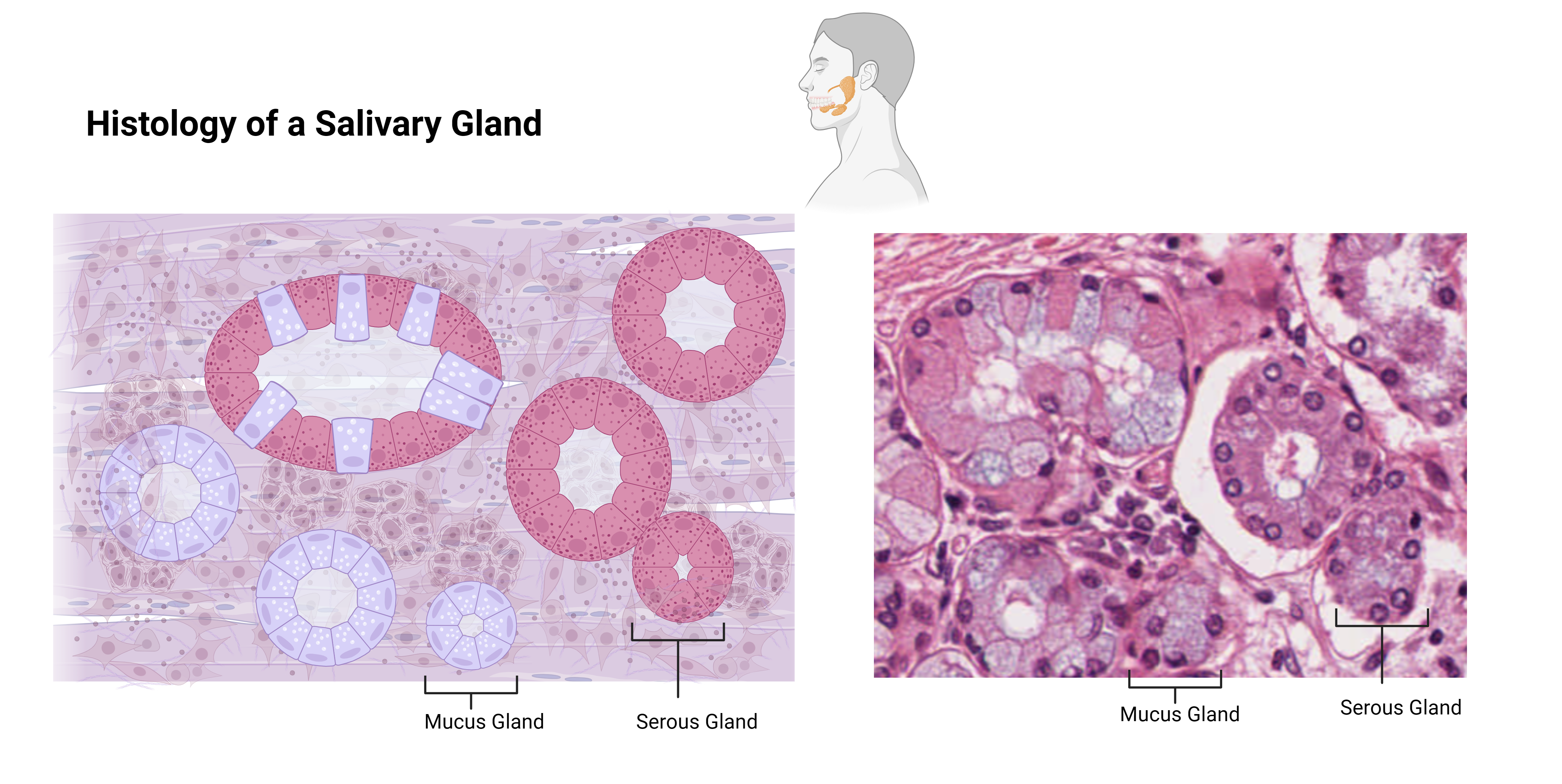
The mouth (oral cavity) is where digestion physically and chemically begins. Teeth break food into smaller pieces (mastication), the tongue manipulates the bolus, and three pairs of salivary glands moisten everything with saliva. Saliva is mostly water, but it also contains amylase (starts starch digestion), lingual lipase (starts fat digestion), lysozyme + IgA (antibacterial), and a buffering bicarbonate.
The mouth is lined by stratified squamous epithelium — same as your skin, but kept moist (non-keratinized) instead of dry. The hard palate and gums are partly keratinized because they take more abrasion; the cheeks and soft palate are non-keratinized.
Submandibular — mixed: mostly serous with mucous tubules (capped by serous demilunes). Produces most of your resting saliva.
Sublingual — almost entirely mucous → thick, slimy saliva.
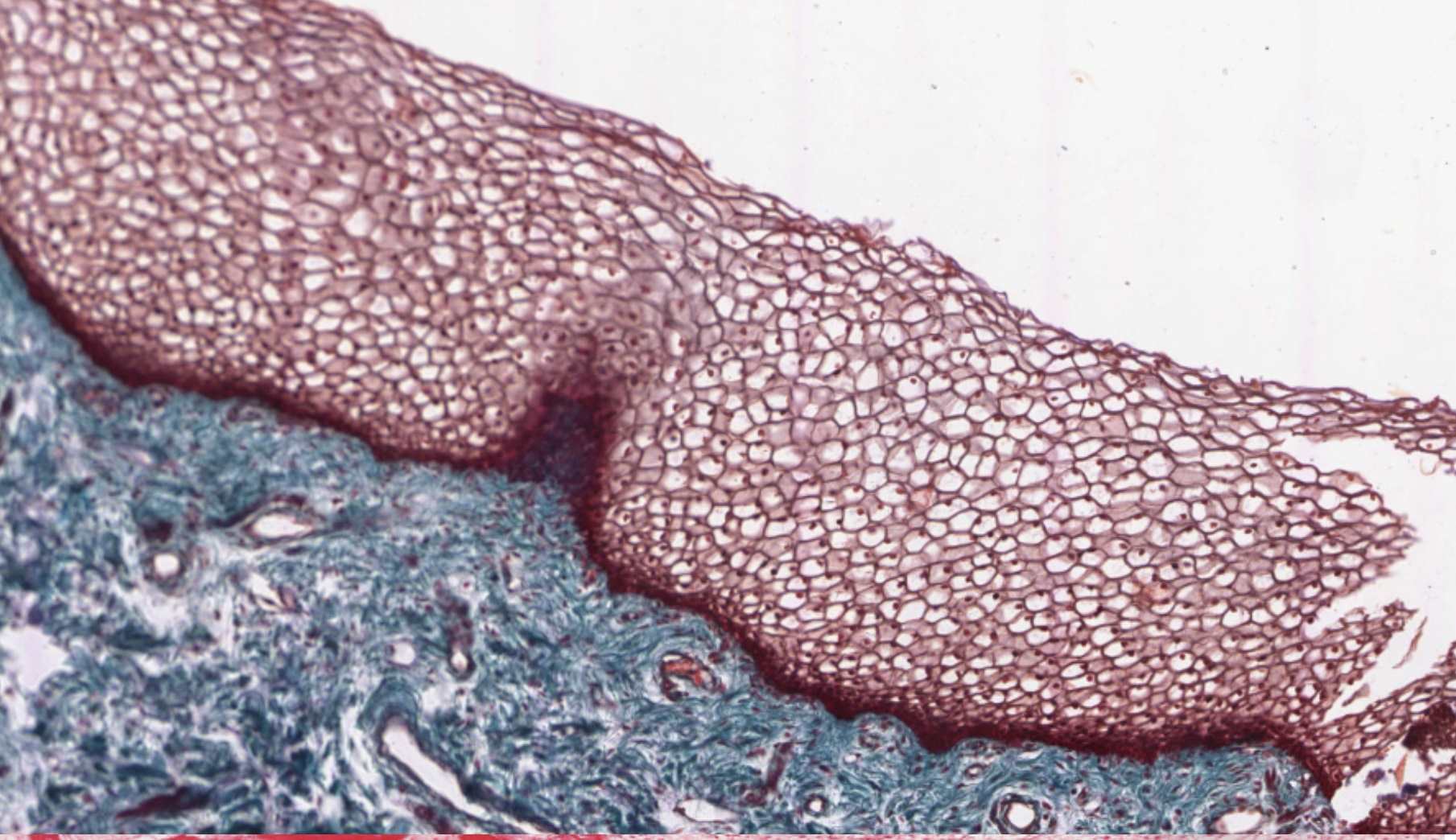
Epiglottis — the swallowing flap
Sitting at the boundary between the oral cavity and the esophagus, the epiglottis is a leaf-shaped flap that flips down over the laryngeal opening when you swallow, sending the bolus toward the esophagus instead of the trachea. Histologically it has a core of elastic cartilage (you can see the dense black-stained elastic fibers between chondrocytes) covered on both surfaces by stratified squamous epithelium that transitions to pseudostratified ciliated columnar on the laryngeal side.

The esophagus — a tube built for the bolus
The esophagus is a 25 cm muscular tube from pharynx to stomach. It does not absorb anything; its only job is to move the bolus from mouth to stomach by peristalsis. So the histology is built around abrasion-resistance and lubrication:
- Stratified squamous lining (same as the mouth — for abrasion).
- Submucosal mucous glands — one of only TWO regions of the gut with submucosal glands (the other is duodenum's Brunner's glands). Their mucus lubricates the bolus.
- Muscularis externa changes along its length: skeletal muscle in the upper third (you can choke yourself voluntarily), mixed in the middle, smooth muscle in the lower third.
- Adventitia on the outside — NOT serosa! The esophagus is OUTSIDE the peritoneal cavity, so it gets a fibrous adventitia instead.
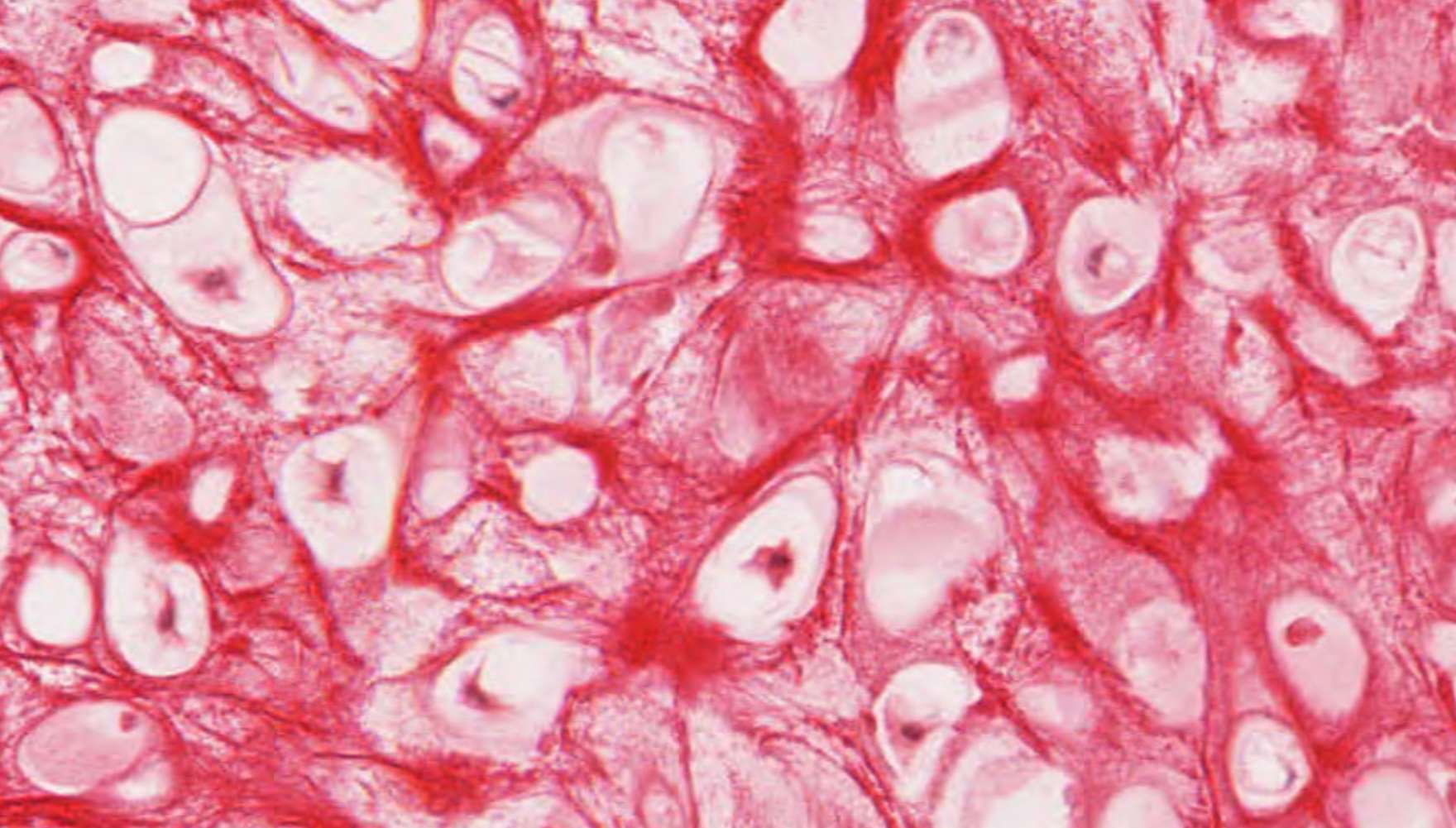
Walking through the esophagus on a slide

The myenteric (Auerbach) plexus. Between the inner circular and outer longitudinal layers of the muscularis externa runs the myenteric plexus — clusters of parasympathetic ganglia and nerve fibers belonging to the enteric nervous system. The myenteric plexus controls peristalsis: when you swallow, this plexus times the wave of muscle contractions that pushes the bolus down into the stomach. The enteric nervous system has more neurons than the entire spinal cord and can run digestive functions independently of the CNS — it is sometimes called the "second brain."


Click to reveal — the swallowing pathway
The first place food (and air) crosses paths is the upper aerodigestive tract. Try to name each numbered structure on the diagram below before clicking the blank to reveal the answer.

- 1click to revealNasal cavity
- 2click to revealHard palate
- 3click to revealTeeth
- 4click to revealTongue
- 5click to revealPharynx
- 6click to revealEpiglottis
- 7click to revealEsophagus
- 8click to revealTrachea
Quick self-check
2 Stomach Day 2 (Tue) • ~25 min • The bag where chemical digestion ramps up ✓
What the stomach actually does
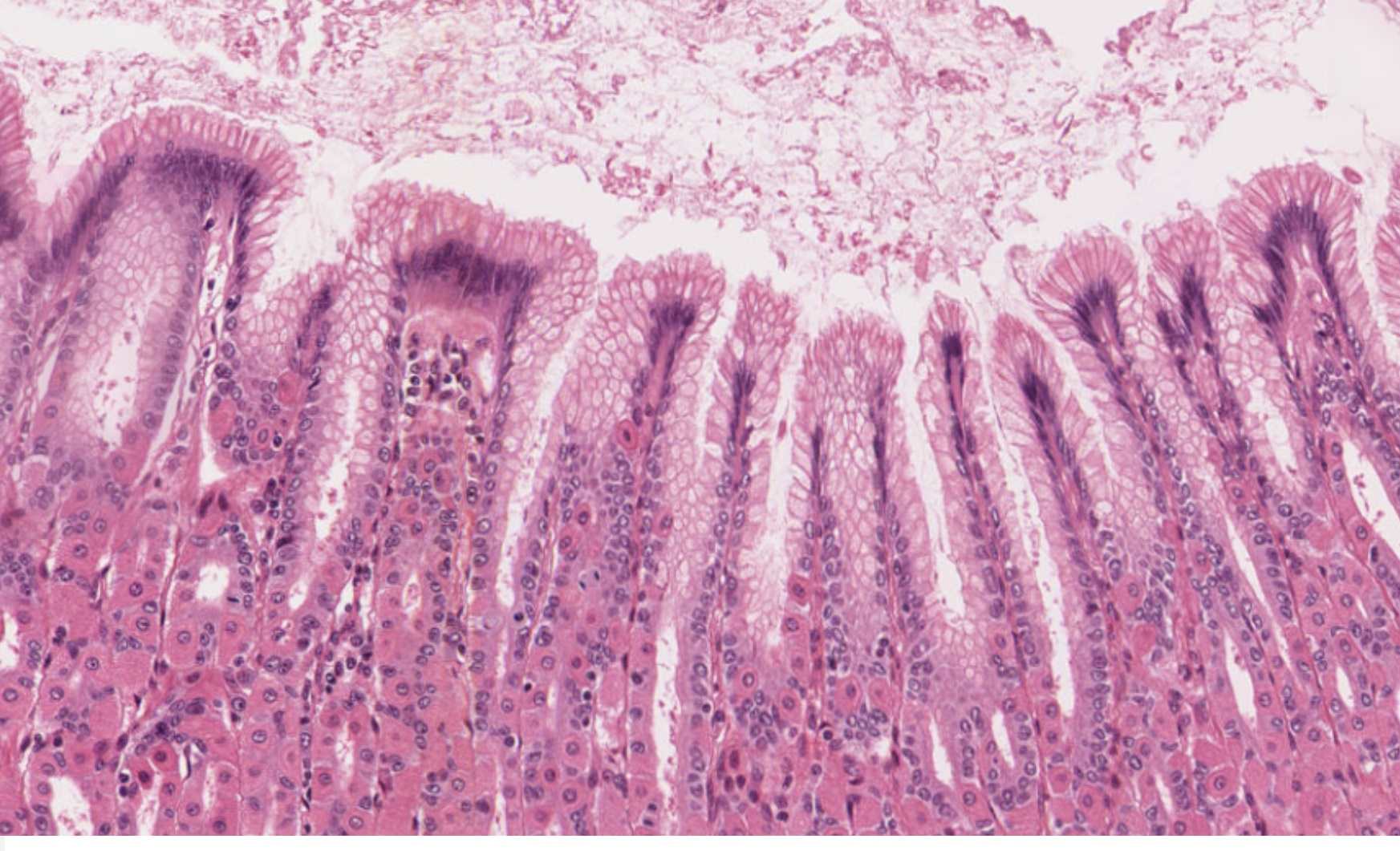
The stomach is a J-shaped sac with three jobs: mechanical mixing (it churns), chemical digestion (HCl + pepsin), and storage (it lets you eat a meal in 15 minutes and digest it over hours). It also kills most swallowed bacteria thanks to its pH of 1.5–2.
The lining changes immediately at the gastroesophageal junction from stratified squamous to simple columnar, and that simple columnar surface dives down into millions of gastric pits. Below each pit, a deeper gastric gland is packed with the cells that do the real work.
Note: the stomach's muscularis externa is unique — it has three layers of smooth muscle (an extra inner oblique layer below the usual circular and longitudinal). This is what lets it churn so vigorously.
Compare cell composition: body region vs. pyloric region
The same simple columnar surface lines the whole stomach, but the cells underneath the pits change as you move from body to pylorus. Use the diagram below to compare the two regions side by side.

Quick self-check
3 Small Intestine Day 3 (Wed) • ~30 min • Where almost all nutrient absorption happens ✓
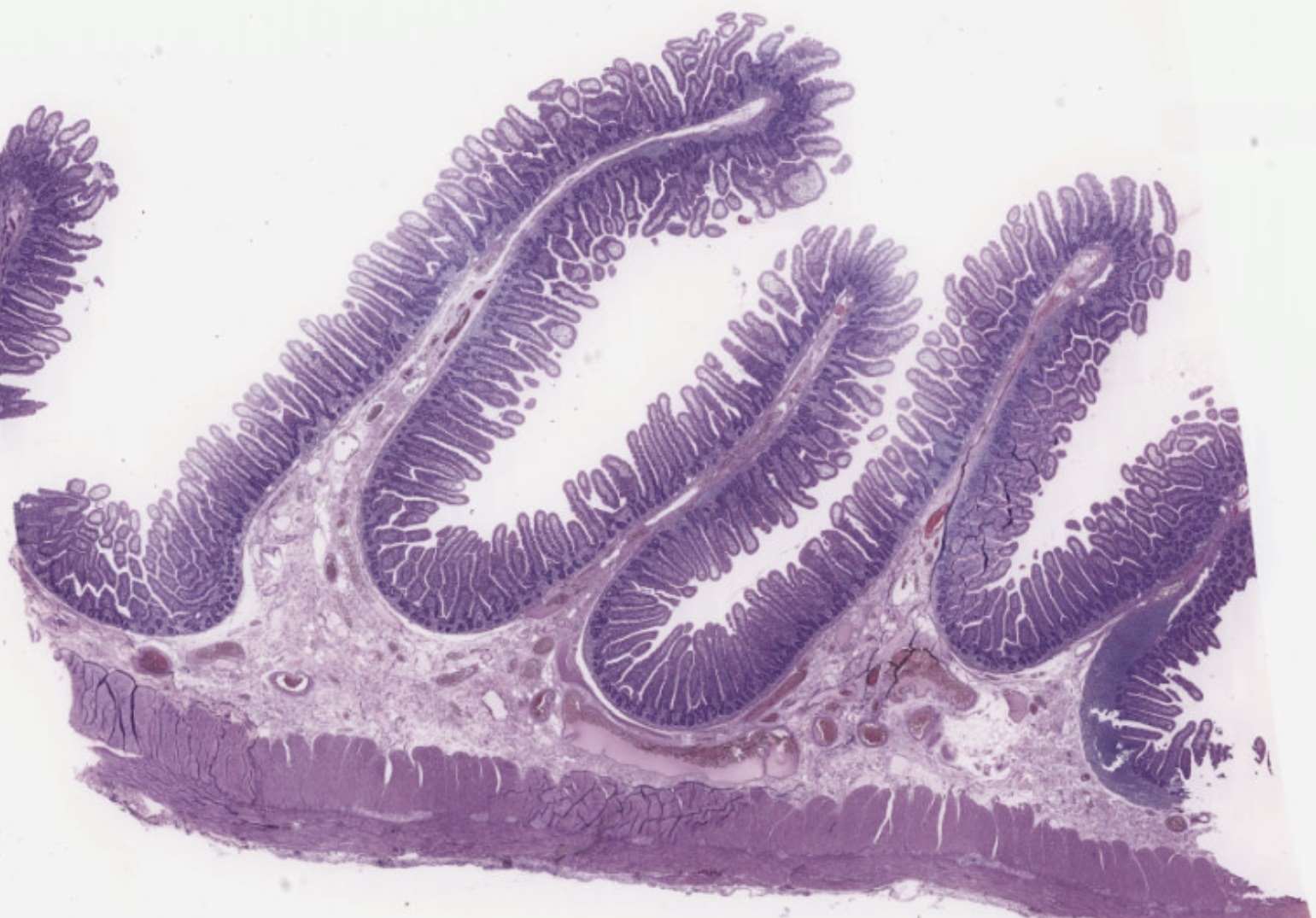
Three levels of surface amplification
To absorb 95% of your day's calories, the small intestine multiplies its surface area roughly 600× over a smooth tube. It does this with three nested levels of folding:
- Plicae circulares — naked-eye circular folds (mucosa + submucosa).
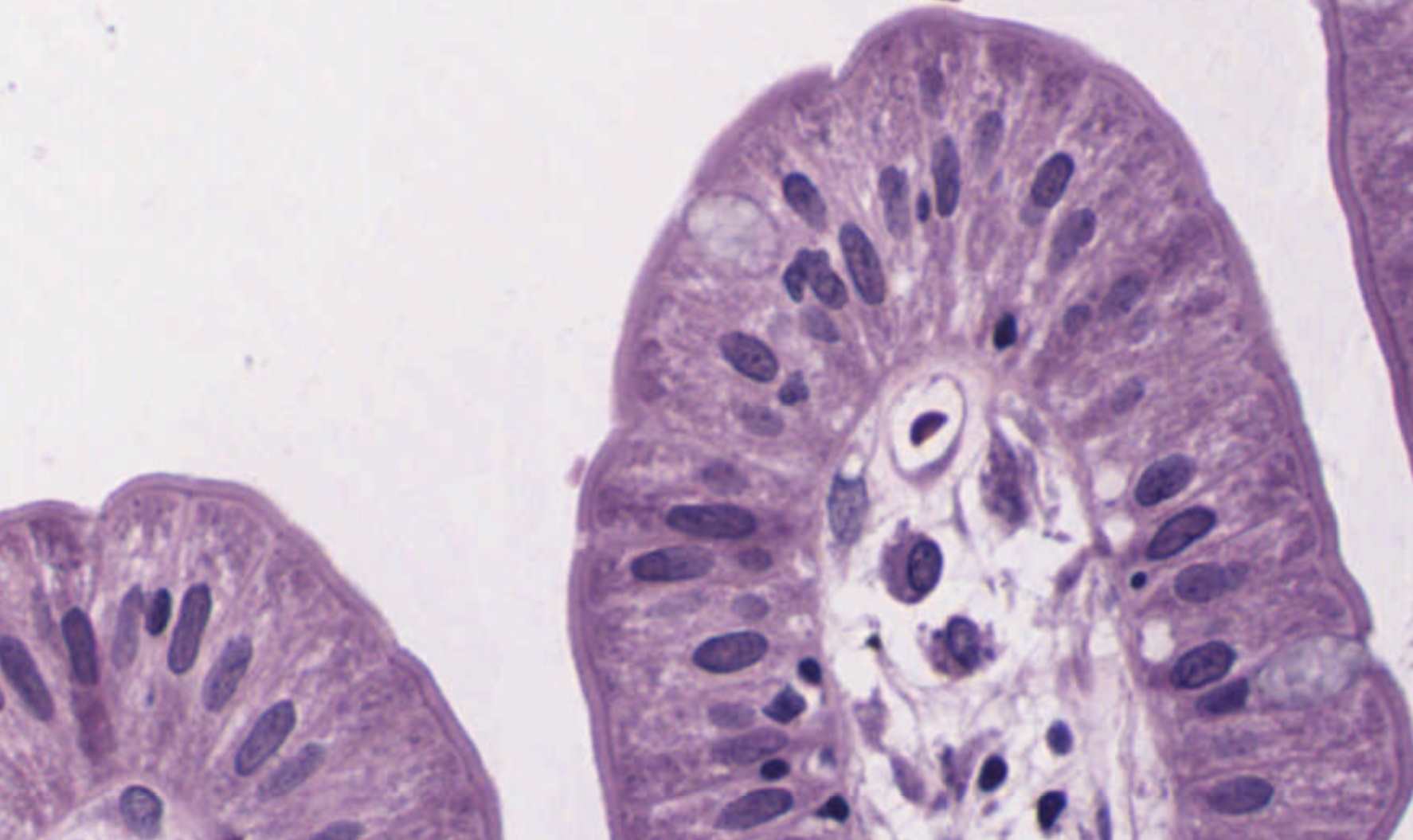
- Villi — finger-like mucosa-only projections (visible at low microscope power).
- Microvilli — the brush border. Only visible by EM, but you can see the fuzzy edge of the apical surface in LM.
Each villus has a central capillary bed (where most absorbed nutrients go into blood) and a single lacteal — a lymphatic capillary that absorbs fats as chylomicrons.
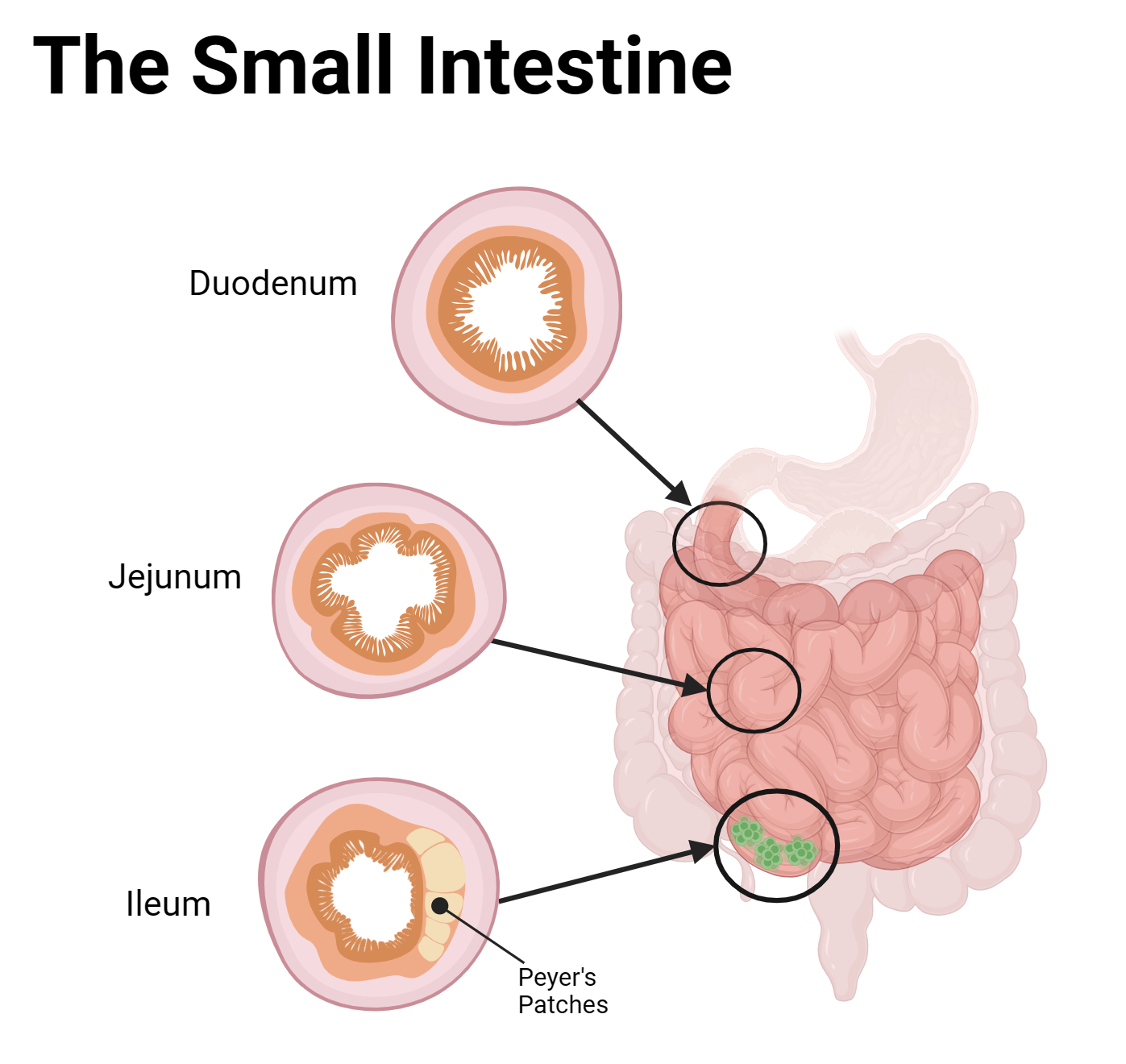
Jejunum — has neither Brunner's nor Peyer's. The "plain" middle subregion. Tallest villi, most plicae circulares.
Ileum — has Peyer's patches: large lymphoid follicles spanning lamina propria AND submucosa. (Bonus stop has more on this.)
Look at the real tissue
Quick self-check
4 Large Intestine, Rectum & Anus Day 4 (Thu) • ~25 min • Water reabsorption + storage; the no-villi region ✓
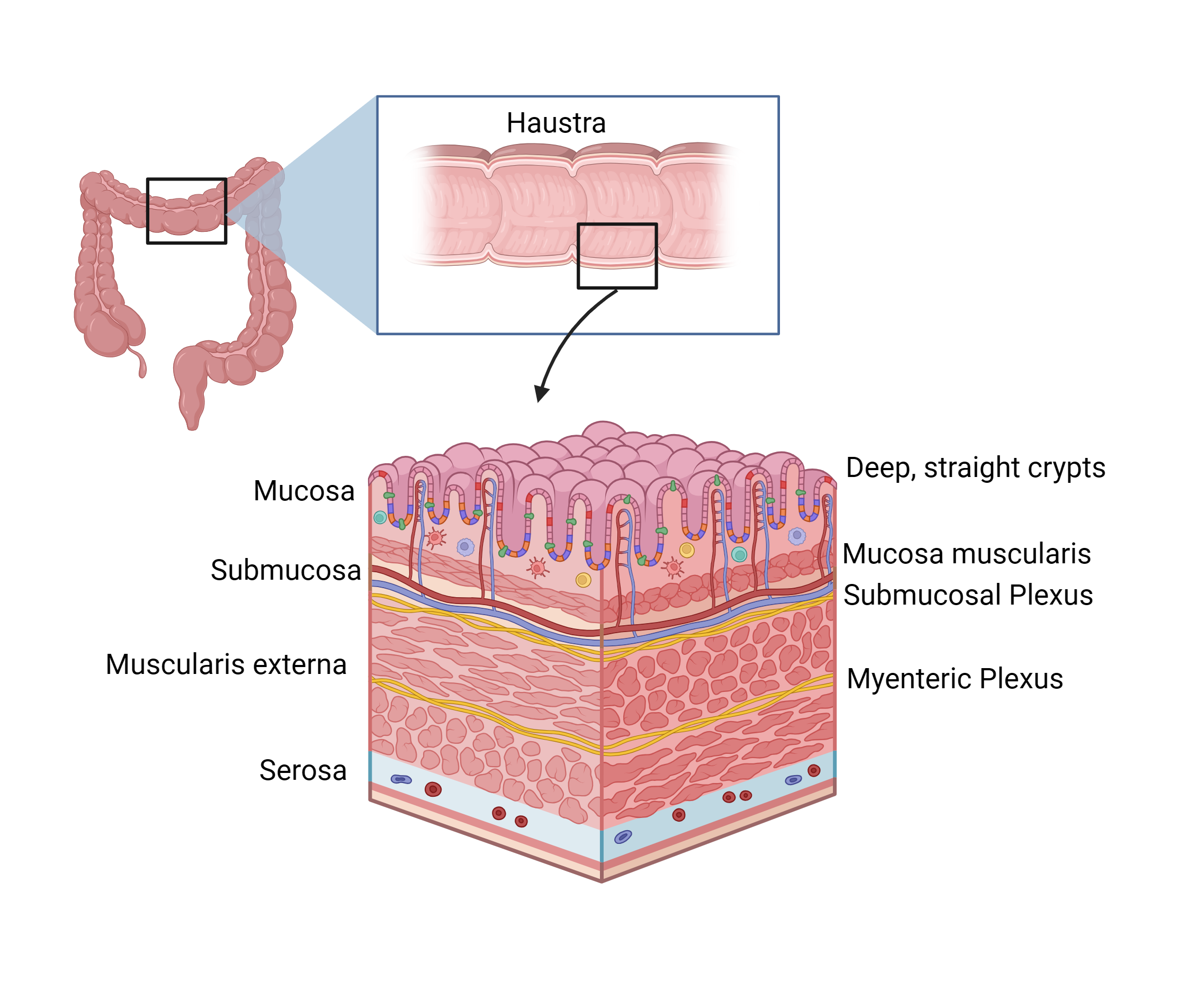
What the colon actually does
By the time material reaches the cecum, almost all the calories are gone. The large intestine has only TWO jobs left: reabsorb water (turning watery chyme into solid stool) and store the residue until you can find a bathroom. So the histology drops the absorptive bells and whistles:
- FLAT mucosal surface — no villi (the most-missed exam point).
- Deep, straight crypts packed with goblet cells. The mucus they make lubricates feces.
- NO Paneth cells (the colon doesn't need them — it's already a thick microbial environment).
- The outer longitudinal muscle is concentrated into THREE thick bands — the taenia coli. Their tonic contraction creates the pouches called haustra.
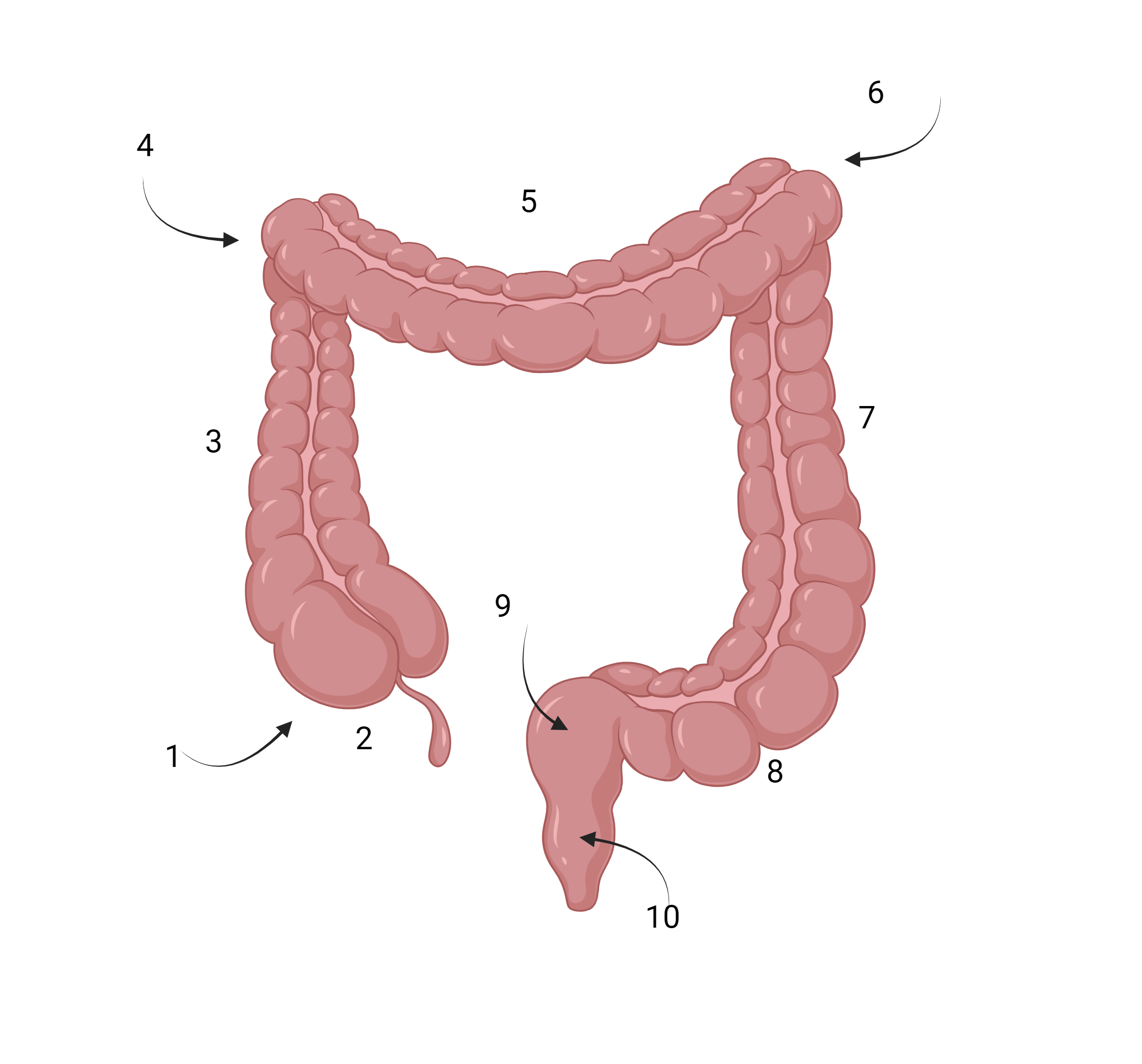
- 1click to revealCecum
- 2click to revealAppendix
- 3click to revealAscending colon
- 4click to revealHepatic flexure
- 5click to revealTransverse colon
- 6click to revealSplenic flexure
- 7click to revealDescending colon
- 8click to revealSigmoid colon
- 9click to revealRectum
- 10click to revealAnal canal
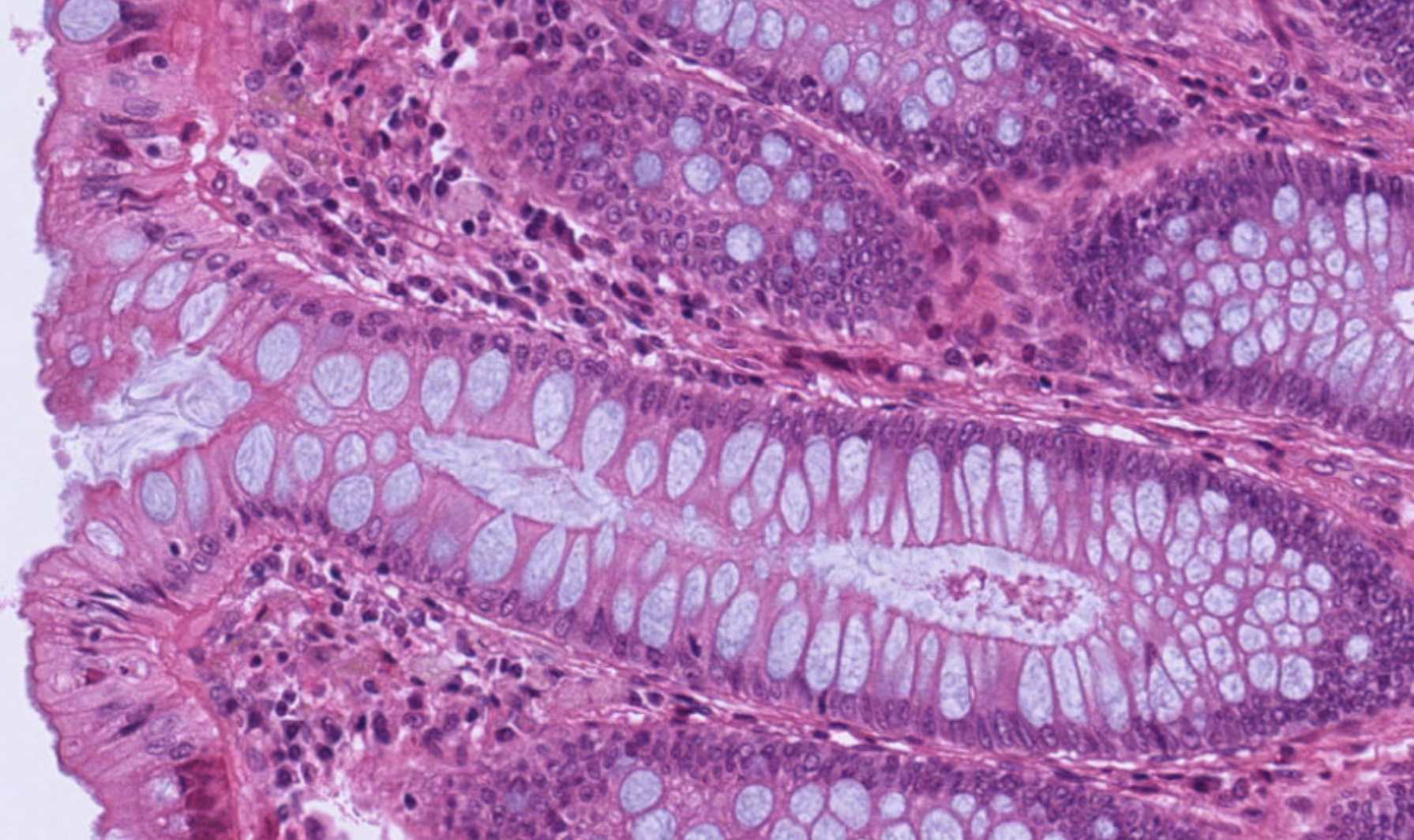
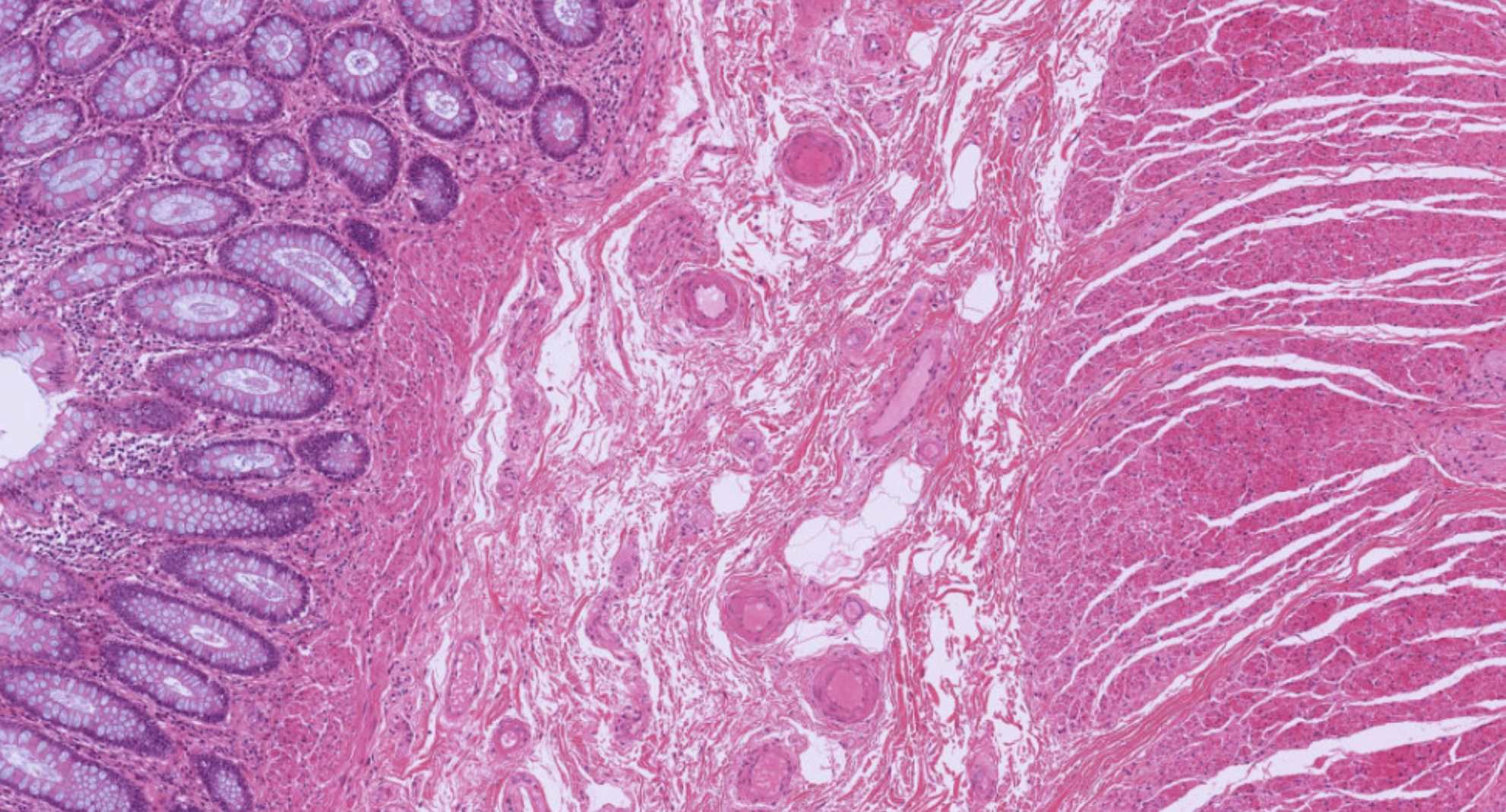
Real tissue — colon mucosa & submucosa
Quick self-check
5 Accessory Glands Day 5 (Fri) • ~30 min • Salivary, pancreas, liver, gallbladder ✓
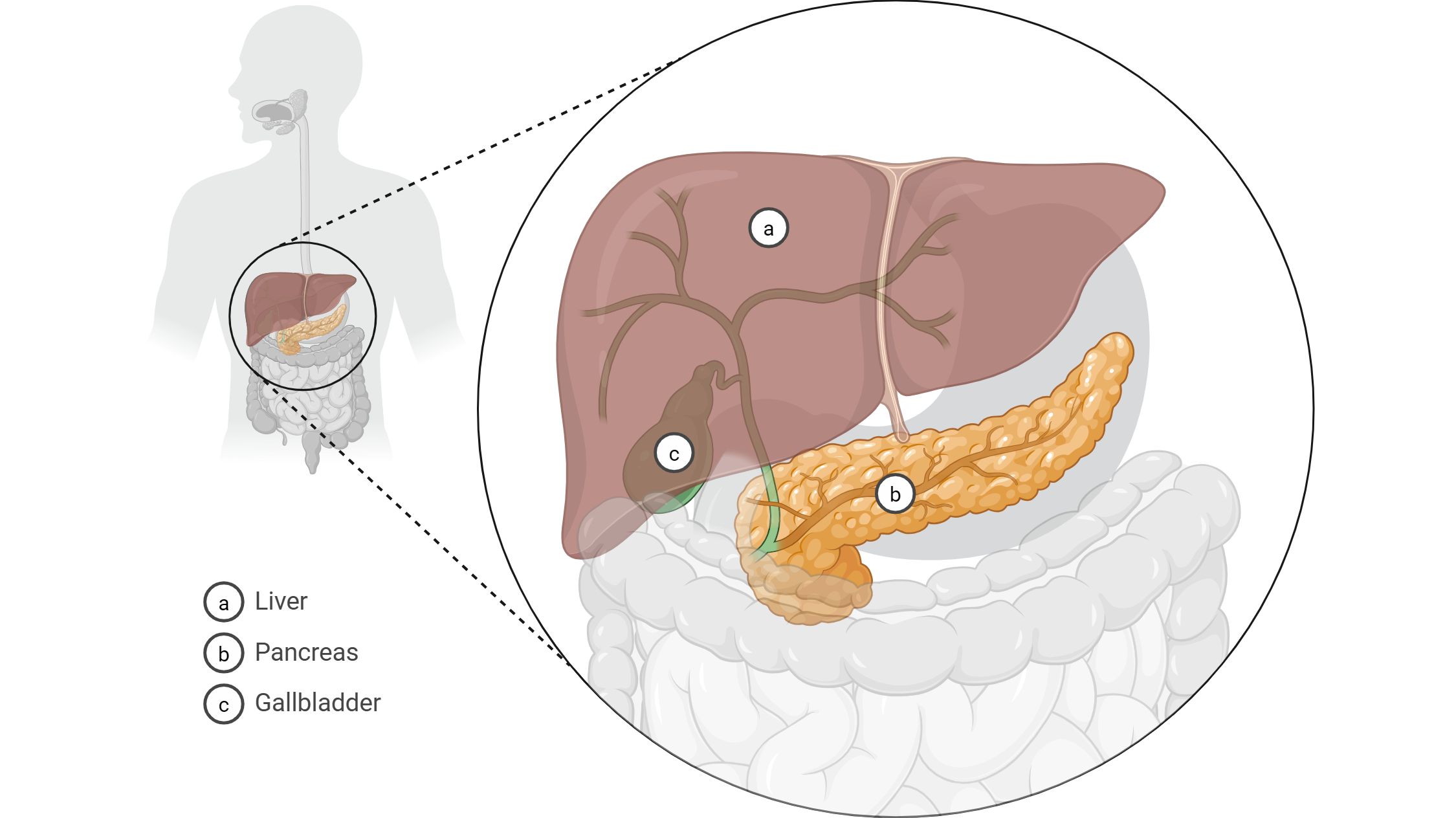
The four accessory glands at a glance
Four organs empty into the digestive tract but are not part of the tube itself: the salivary glands (into the mouth) and the pancreas, liver, and gallbladder (all into the duodenum). The pancreas and gallbladder ducts often join to form the hepatopancreatic ampulla just before they empty.


Quick self-check
6 BONUS — Immune Structures (GALT/MALT) Weekend (extra) • ~25 min • Adenoids, MALT, appendix, and Peyer's patches ✓
Why the gut is the immune system's biggest neighborhood
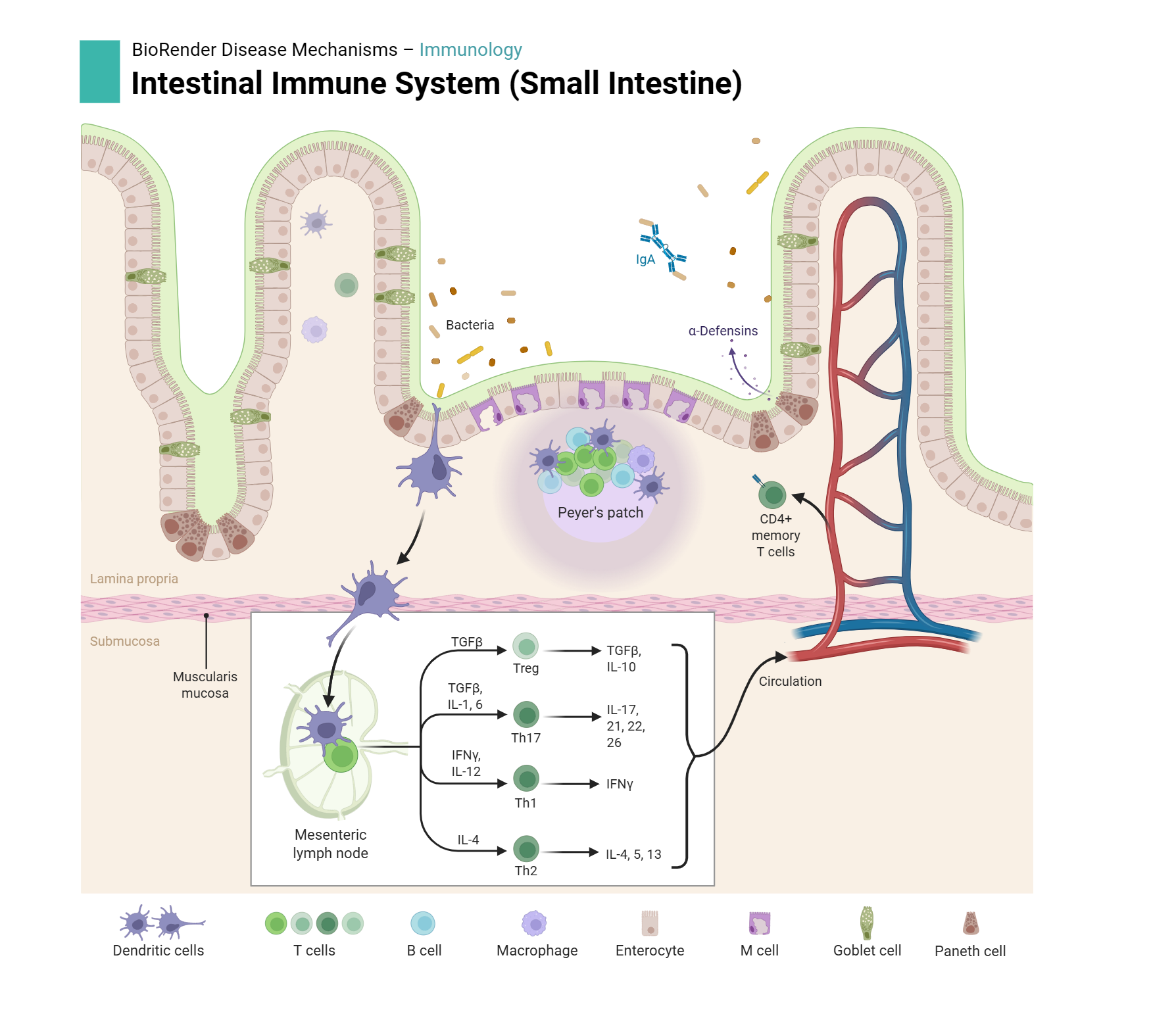
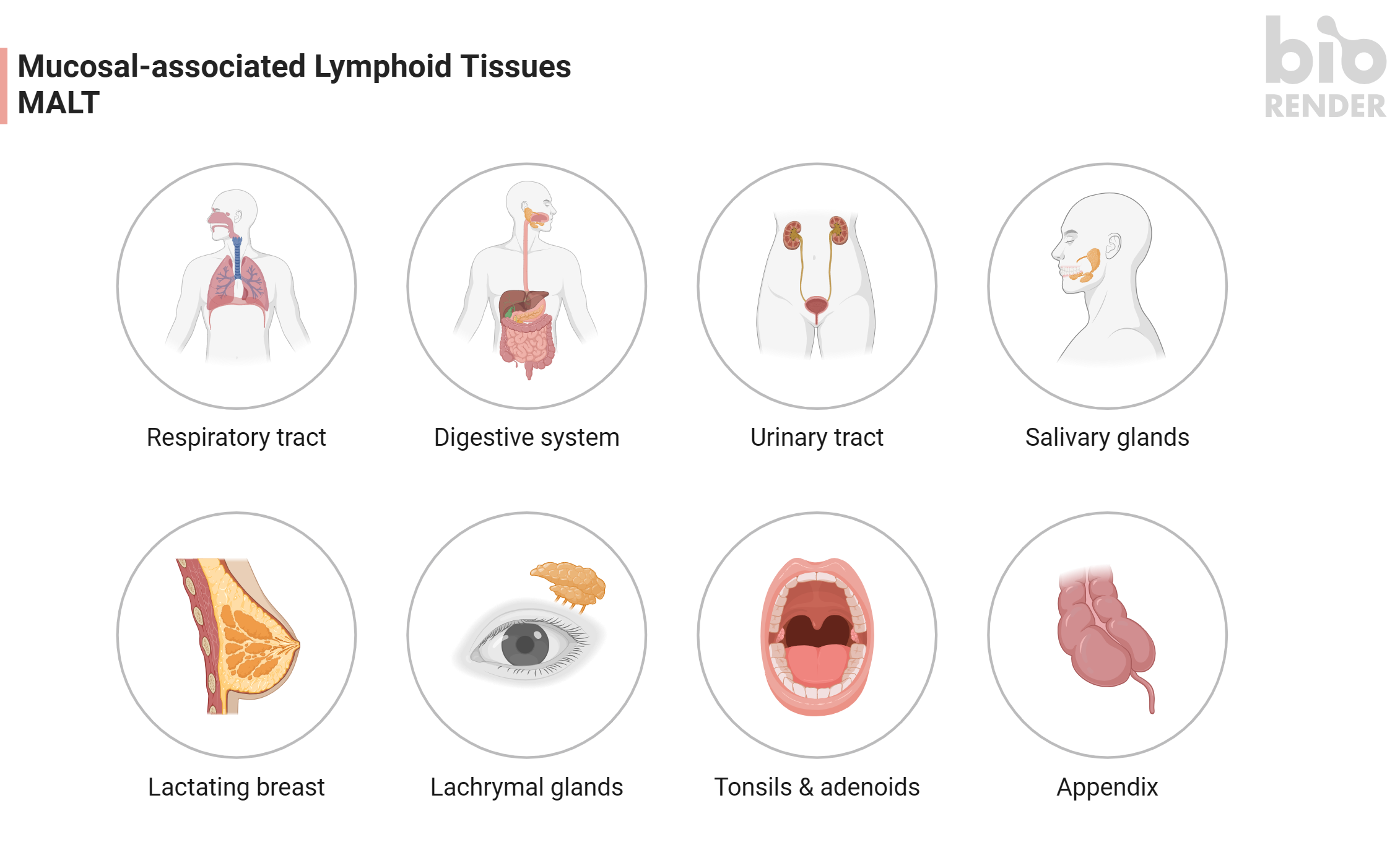
By surface area, the digestive tract is the body's largest interface with the outside world — bigger even than the skin. Every meal carries food antigens AND a population of swallowed microbes. To handle that without constantly being inflamed, the gut wall has lymphoid tissue at every level. Together this is called GALT (gut-associated lymphoid tissue), part of the larger MALT (mucosa-associated lymphoid tissue) network. GALT contains roughly 70% of all the lymphocytes in your body.
The named GALT/MALT structures
Pharyngeal tonsils (adenoids) — back of the nasopharynx; pseudostratified ciliated columnar epithelium over follicles.
Palatine tonsils — between the palatoglossal and palatopharyngeal arches; stratified squamous + deep crypts diving into lymphoid tissue.
Lingual tonsils — at the root (back) of the tongue.
Note: the muscularis mucosae is INTERRUPTED beneath each patch — necessary so cells can move between mucosal and submucosal halves of the follicle.
Clinical aside: patients with selective IgA deficiency get more frequent gut and respiratory infections. Patients on long-term steroids have shrunken Peyer's patches and similar problems. Nurses see this every day on transplant and rheumatology services.
Click to reveal — Peyer's patch structures
Quick self-check
Quick decision card — when in doubt at the scope
If you put an unknown slide on the scope, ask three questions in this order:
1. What is the lining? Stratified squamous = esophagus or anal canal. Simple columnar = stomach, small intestine, or colon.
2. If simple columnar, are there villi? Yes = small intestine. No = stomach (look for pits + parietal/chief cells) or colon (flat surface, many goblet cells).
3. If small intestine, do I see Brunner's or Peyer's? Brunner's (submucosal mucous glands) = duodenum. Peyer's (large lymphoid follicles) = ileum. Neither = jejunum.
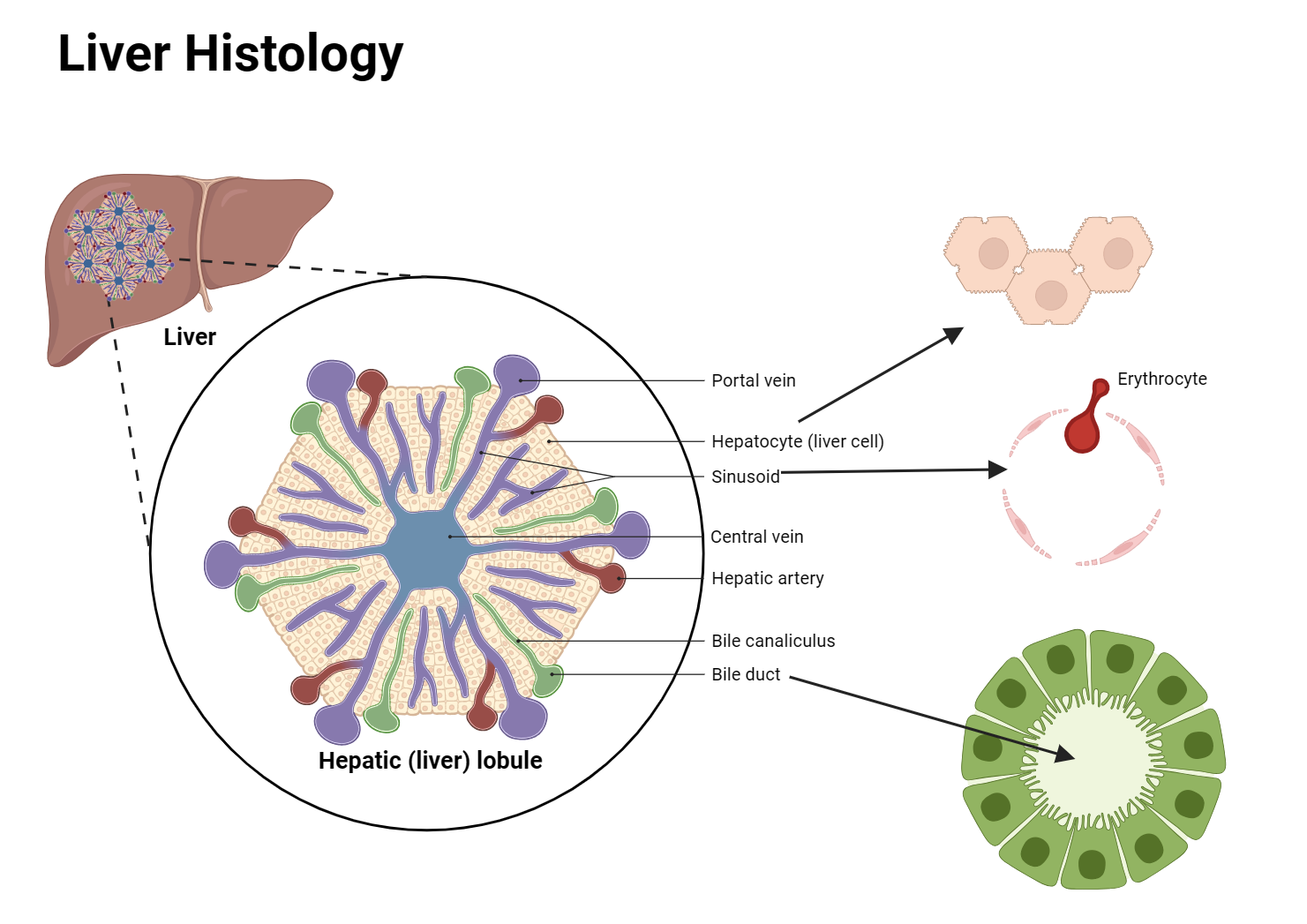
For accessory glands, look for the signature features: salivary = mixed acini; pancreas = acini + pale islet; liver = hexagonal lobule with central vein; gallbladder = tall folds with no submucosa.