How to use this page
This journey covers the urinary system from gross kidney down to the bladder wall, in five stops spread across one week. Each stop takes about 20–30 minutes and follows the same rhythm:
- A little reading to set the scene.
- A little interaction (H5P activities embedded in your course page; click-to-reveal labeling here).
- A little confirmation — a mini self-check.
One topic per day, organized so the toughest skill (telling tubules apart) gets two full stops:
- Stop 1 — Mon. Map the kidney from outside in. Cortex, medulla, calyces, and the renal pelvis (renal basin).
- Stop 2 — Tue. The glomerulus. The filtering ball and the parts of the renal corpuscle.
- Stop 3 — Wed. PCT & nephron loop. The first half of the nephron's tubule path.
- Stop 4 — Thu. DCT & Collecting duct. The second half — and the trickiest tubules to tell apart.
- Stop 5 — Fri. Drainage & storage. Renal pelvis details, ureter, bladder, and transitional epithelium.
Click any stop to expand. Progress is saved automatically in this browser.
1 Map the territory Mon • ~25 minutes • Cortex / medulla / calyx / renal basin / ureter ✓
The kidney from outside in
The kidney has two jobs and the tissue is split between them. The cortex is the outer band — that's where the filtering happens, in millions of tiny units called nephrons. The medulla is the inner triangular region, organized into renal pyramids. The medulla concentrates the filtrate as it drains downward.
Each pyramid points inward, with its tip — the renal papilla — opening into a small cup called a minor calyx. Several minor calyces merge into a major calyx, and all the major calyces drain into the central reservoir of the kidney: the renal pelvis, also called the "renal basin". From there, urine leaves through the ureter.
Two terms, one structure: renal pelvis = renal basin. Different textbooks use different names. Recognize both.
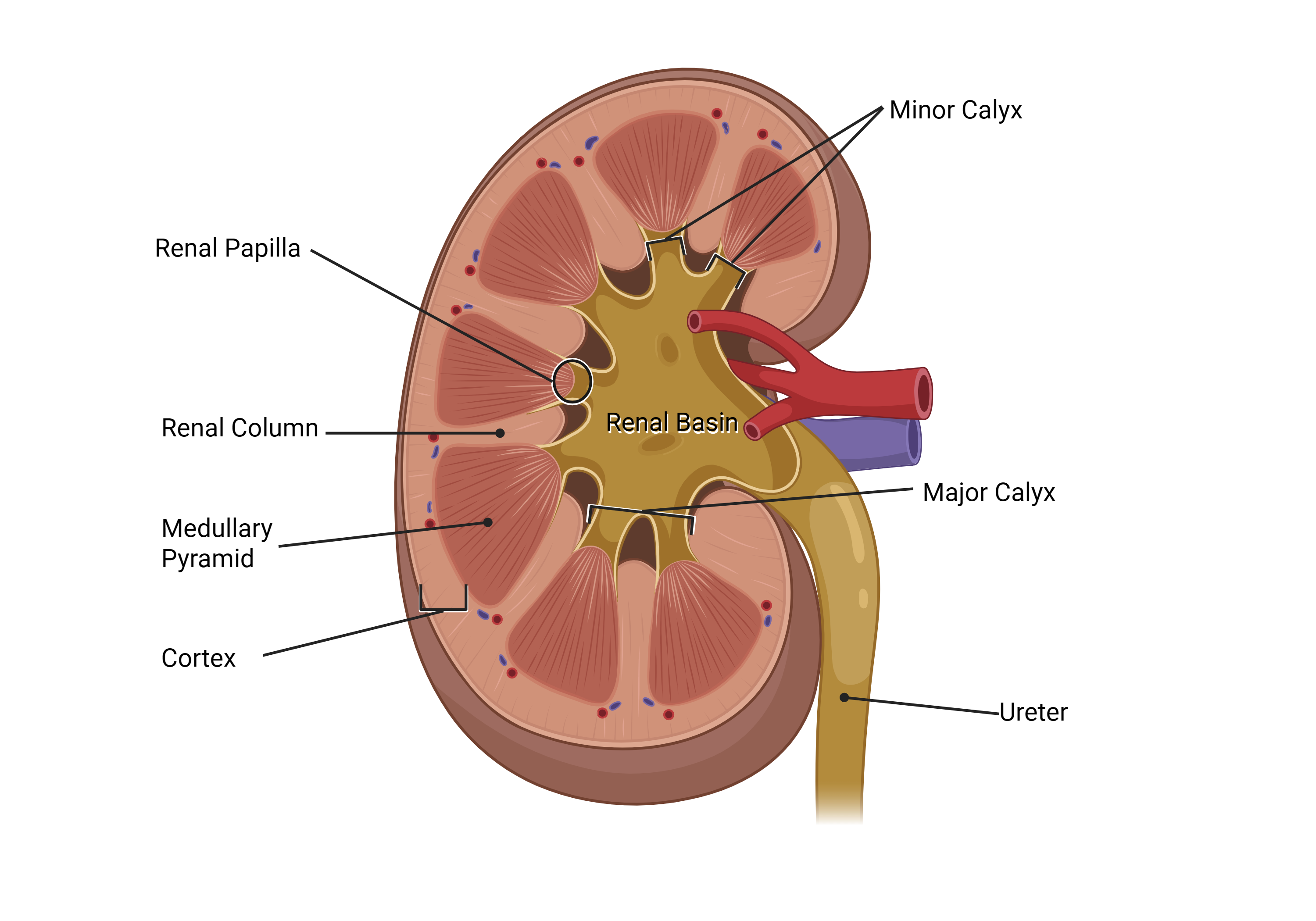
Click to reveal — the kidney parts
Try to name each numbered structure on the diagram below before clicking the blank to reveal the answer.

- 1click to revealCortex
- 2click to revealMedulla (renal pyramid)
- 3click to revealRenal column
- 4click to revealRenal papilla
- 5click to revealMinor calyx
- 6click to revealMajor calyx
- 7click to revealRenal pelvis ("renal basin")
- 8click to revealUreter
Quick self-check
2 The glomerulus & renal corpuscle Tue • ~20 minutes • The filter at the start of every nephron ✓
What is a renal corpuscle?
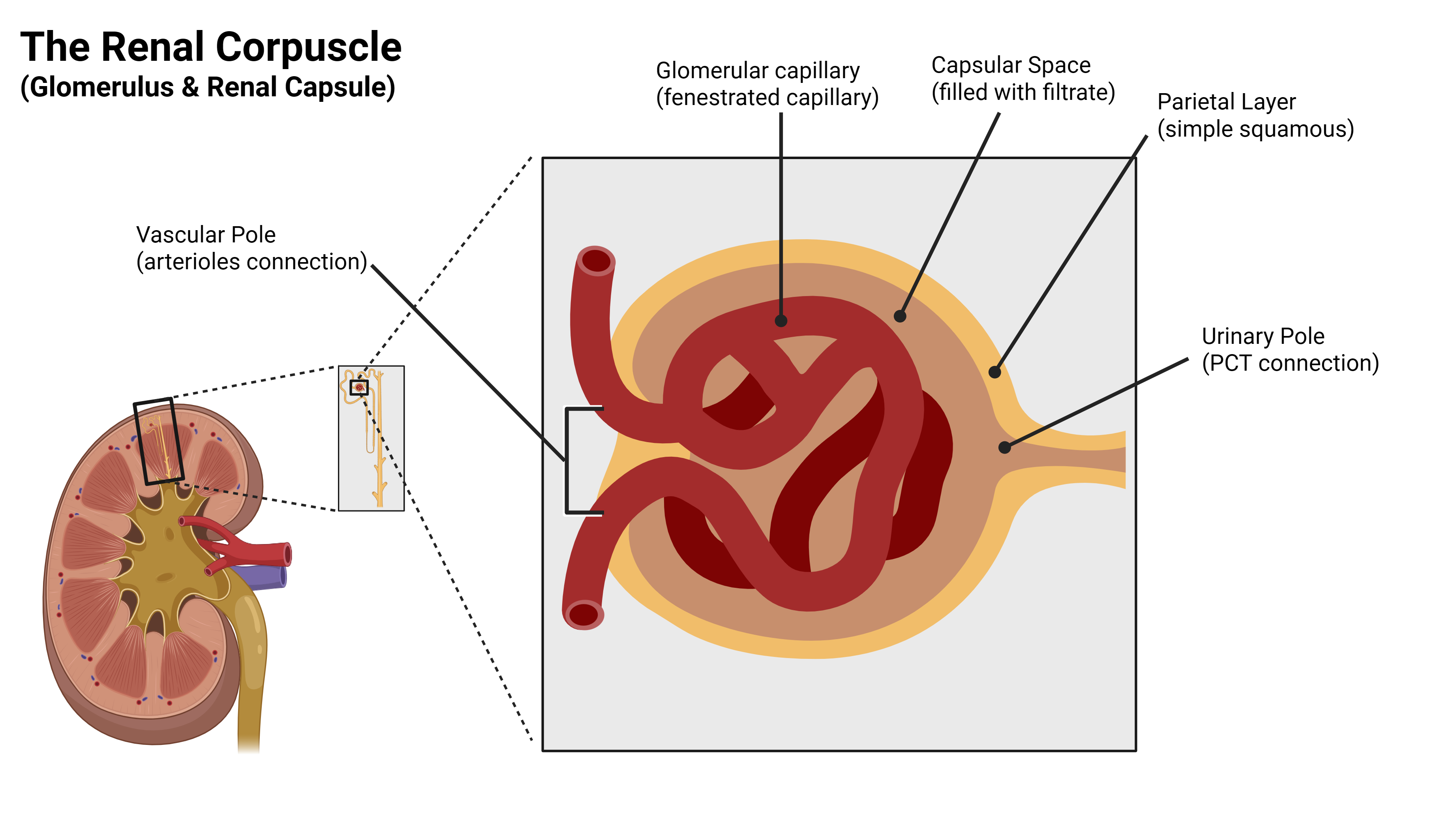
A renal corpuscle is the filtering apparatus at the start of each nephron — about a million of them per kidney. It has two parts that fit together like an egg in a cup:
- The glomerulus — a tangled ball of capillaries.
- The glomerular capsule (renal capsule) — a hollow cup wrapped around the glomerulus.
Blood enters the glomerular capillaries under pressure. Plasma (and small dissolved things — water, salts, glucose, amino acids, urea) is forced ACROSS the capillary wall into the hollow space inside the capsule. Cells and large proteins are too big to cross, so they stay in the blood.
The three parts on the curriculum list
Now look at a real glomerulus
Move from the schematic to a real micrograph. Find the glomerular capillary tuft, the capsular space around it, and the thin parietal layer.
Click to reveal — the renal corpuscle
Name each part of the corpuscle before revealing the answer.

- 1click to revealGlomerular capillaries
- 2click to revealCapsular space
- 3click to revealParietal layer (simple squamous)
- 4click to revealUrinary pole (filtrate exits to PCT)
- 5click to revealVascular pole (afferent in / efferent out)
Quick self-check
3 PCT & nephron loop Wed • ~30 minutes • The first half of the nephron tubule path ✓
The first half of the journey: PCT → Loop
Filtrate exits the corpuscle and immediately enters the Proximal Convoluted Tubule (PCT), which winds around for a while in the cortex doing the bulk of reabsorption. Then it dives down into the medulla as the descending limb of the nephron loop, makes a hairpin turn, and rises back up to the cortex.
PCT — the workhorse of reabsorption
The PCT reabsorbs about two-thirds of everything in the filtrate: water, glucose, amino acids, sodium, bicarbonate, most small ions. To do that much work, the apical surface of each PCT cell is covered in microvilli — collectively called the brush border. The brush border is what makes the PCT lumen edge look fuzzy or out-of-focus under the microscope.
What you see: simple cuboidal cells with a fuzzy/blurry lumen edge from the brush border (microvilli). Few sparse round nuclei.
Watch out for: easy to confuse with DCT — both are simple cuboidal in the cortex. The brush border is the one feature that reliably tells them apart.
Nephron loop — the medullary U-turn
From the PCT, filtrate enters the descending limb of the loop and travels straight DOWN into the medulla. The descending limb is permeable to water — water leaves the tubule, and the filtrate inside becomes more concentrated.
At the bottom of the loop, the tubule makes a hairpin turn and becomes the ascending limb, traveling straight UP back into the cortex. The thin part of the ascending limb is permeable to salt — salt leaves the tubule, and the filtrate becomes more dilute.
Together, the descending and ascending limbs build the salt gradient in the medulla that makes urine concentration possible later, in the collecting duct.
What you see: very thin wall, almost flat — simple squamous epithelium. Looks like a capillary, but with no red blood cells inside.
Watch out for: students often mistake thin loops for capillaries. Trick: capillaries have RBCs; thin loops don't.

Side-by-side comparison
| Tubule | Region | Epithelium | ID give-away |
|---|---|---|---|
| PCT | Cortex | Simple cuboidal | Fuzzy lumen edge from brush border; few sparse round nuclei |
| Nephron loop (thin) | Medulla | Simple squamous | Almost flat; looks like a capillary but no RBCs inside |
The first two steps of the decision card
For PCT & Loop, ask in this order:
Now look at real tissue
The schematic teaches you what to expect; real micrographs are what you'll be tested on. Compare these to the schematic above.
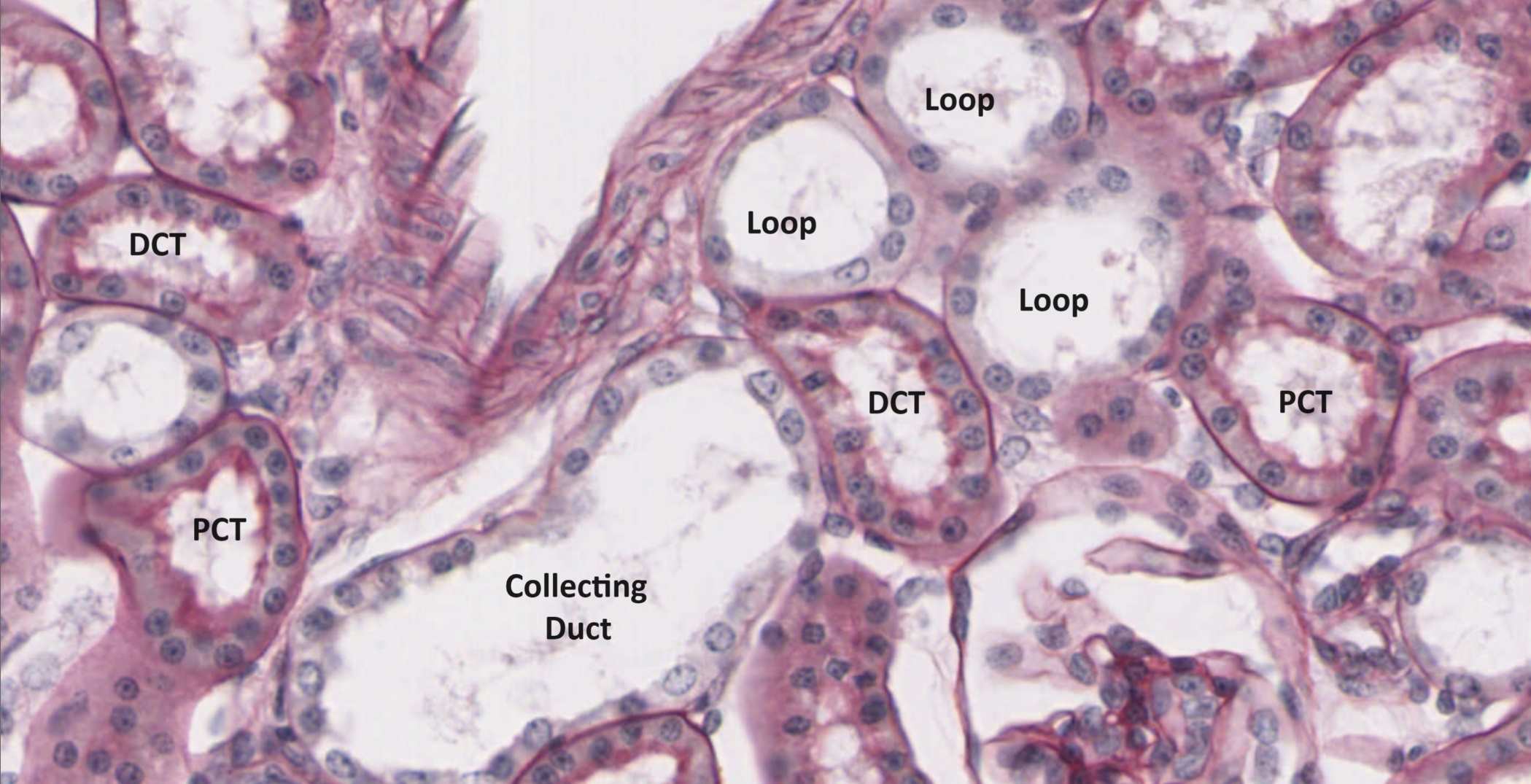
Kidney slide #210, PAS stain, labeled tubules. The PAS stain highlights the brush border on the apical surface of PCT cells — that's what makes those lumen edges look fuzzy on H&E too.
Kidney slide #206, medulla, labeled nephron loop. Notice how thin the wall is — almost flat. The nuclei sit ON the wall like beads on a string.
Click to reveal — the nephron path
Find the PCT and the descending and ascending limbs on the labeled nephron.

- 1click to revealGlomerular capillaries
- 2click to revealCapsular space
- 4click to revealPCT
- 5click to revealNephron loop (descending)
- 6click to revealNephron loop (ascending)
- 7click to revealDCT (covered tomorrow)
- 8click to revealCollecting duct (covered tomorrow)
Quick self-check
4 DCT & Collecting duct Thu • ~30 minutes • The trickiest tubules to tell apart ✓
The second half of the nephron: DCT → CD
After the nephron loop, filtrate enters the Distal Convoluted Tubule (DCT), which winds around briefly in the cortex doing fine-tuning under hormonal control. From there, several DCTs from many nephrons all dump into a shared collecting duct. The collecting duct travels straight DOWN through the medulla and opens at the renal papilla.
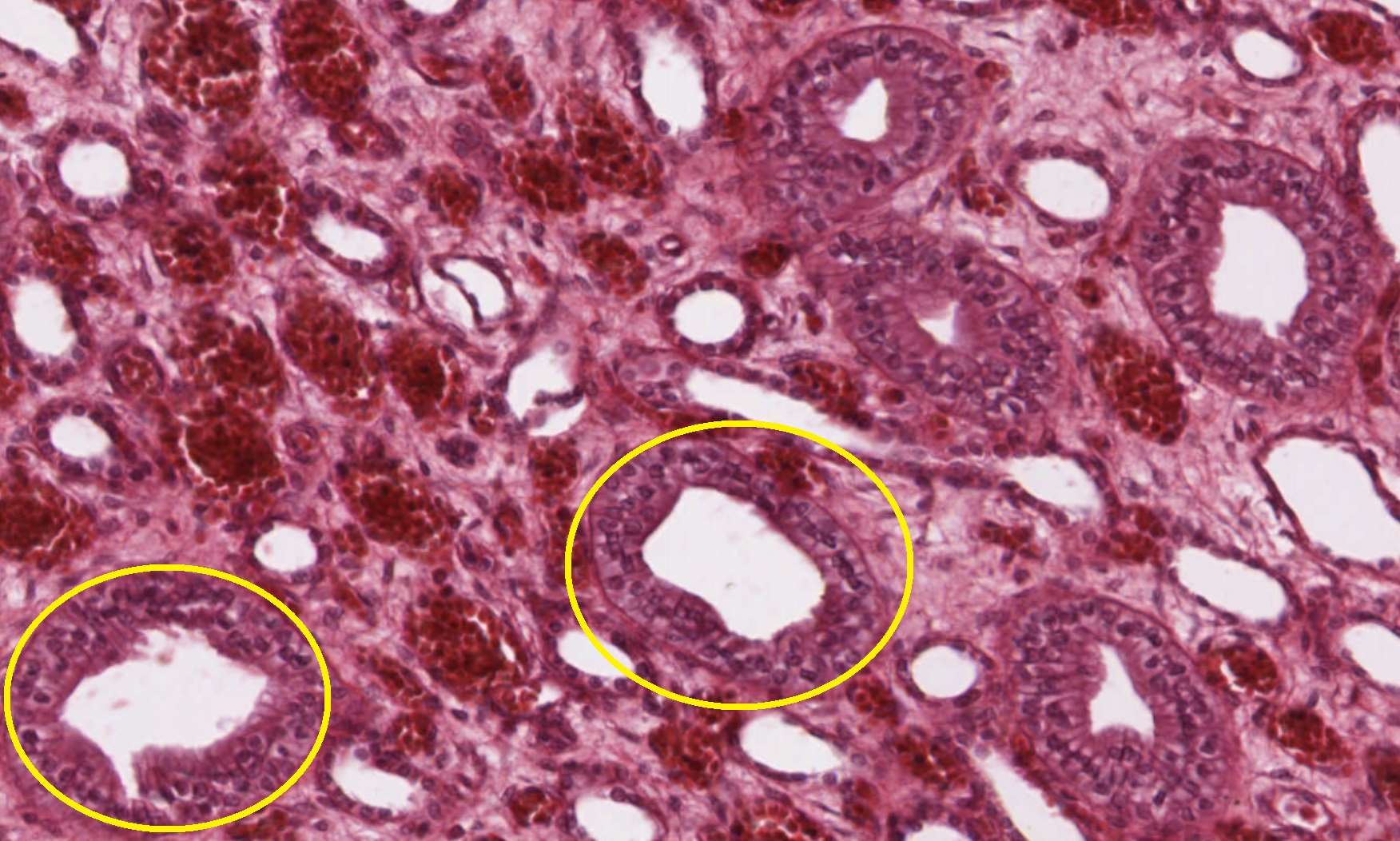
DCT — the fine-tuner
The DCT is shorter than the PCT and its cells are smaller, so a cross-section packs in more nuclei per unit area. There's no brush border, so the lumen edge is sharp and clean.
The DCT does the fine-tuning of urine composition under hormonal control: aldosterone tells it to reabsorb more sodium (and dump potassium); parathyroid hormone tells it to reabsorb more calcium.
What you see: simple cuboidal cells with a sharp, clean lumen edge. Many crowded nuclei toward the lumen.
Watch out for: vs. PCT — DCT is missing the brush border, that's the call. vs. collecting duct — DCT cell borders are less distinct.
Collecting duct — the final shaper
Collecting ducts are the last stop before urine leaves the kidney. They're under control of antidiuretic hormone (ADH): when ADH is high (you're dehydrated), the collecting ducts become permeable to water — water leaves and you make small amounts of concentrated urine. When ADH is low (well hydrated), water stays in the duct and you make lots of dilute urine.
Histologically, the giveaway is the clarity of cell borders. You can usually see the membrane between adjacent cells — something that's much harder to spot in the PCT or DCT. The cells are also taller (cuboidal that grades into columnar as the duct descends through the medulla).
What you see: sharp lumen edge + you can clearly see EACH cell's outline. Cleaner-looking than PCT or DCT. Bigger, fewer cells.
Watch out for: in the medulla, you'll see lots of these in parallel. Don't confuse with thin loops (those are squamous, much smaller).

All four tubules — the full decision card
Now that you've met all four tubules, here's the complete decision rule. Use it on every cortex and medulla micrograph for the rest of the unit.
Tubule ID — ask in this order. The first YES wins.
All four tubules side-by-side
| Tubule | Epithelium | ID give-away |
|---|---|---|
| PCT | Simple cuboidal | Fuzzy lumen edge from brush border; few sparse round nuclei |
| DCT | Simple cuboidal | Sharp lumen edge; many crowded nuclei toward the lumen |
| Collecting duct | Simple cuboidal → columnar | Sharp lumen + distinct cell borders (you can see each cell) |
| Nephron loop (thin) | Simple squamous | Almost flat; looks like a capillary but no RBCs inside |
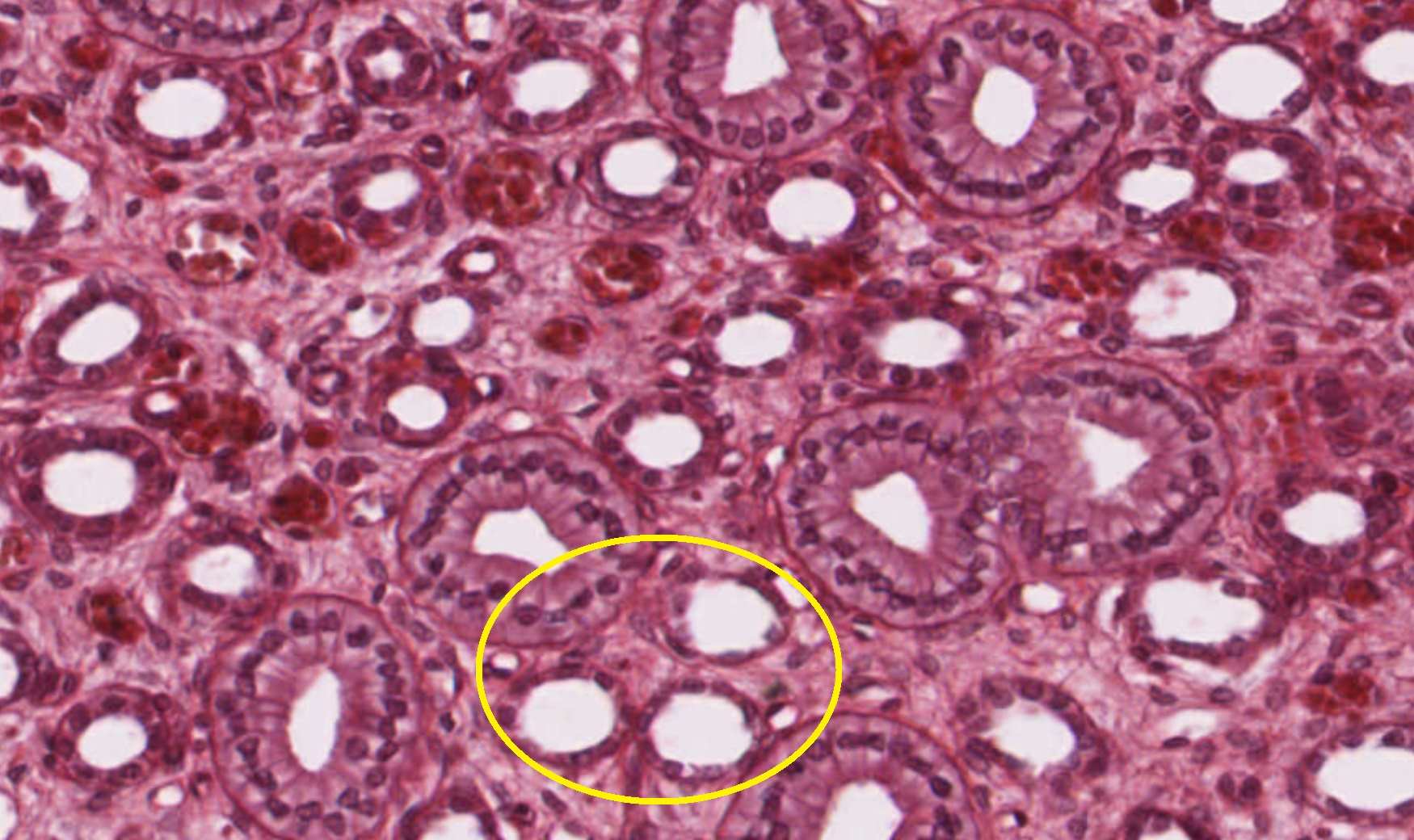
Now look at real collecting ducts
Two micrographs from different slides. Both show the parallel-tube view of the medulla. Look for the distinct cell borders that mark the collecting ducts — and notice the smaller, thinner-walled tubes near them are the nephron loops.

Slide #210 — collecting ducts labeled in the renal medulla.
Slide #206 — a different field of medulla, again with collecting ducts called out. The cell borders are the giveaway.
Quick mental practice — name the tubule
Cover the labels on the four-tubule diagram above and try to ID each one before peeking. When you can do all four without hesitation, you're ready for the H5P question set.
Quick self-check
5 Drainage & storage — ureter and bladder Fri • ~25 minutes • Renal basin details, ureter, transitional epithelium, detrusor ✓
From the renal basin to the bladder
Once urine leaves the collecting duct at the renal papilla, it's done being made — now it just needs to get out. The plumbing path:
renal papilla → minor calyx → major calyx → renal pelvis ("renal basin") → ureter → bladder → urethra
The ureter and bladder share a two-feature signature: transitional epithelium on the inside, smooth muscle outside. The smooth muscle moves urine along the ureter (peristalsis) and squeezes the bladder during urination (the detrusor muscle).
Transitional epithelium — the shape-shifter
Transitional epithelium is unique. It changes shape with stretch:

Click to reveal — the bladder wall

- 1click to revealLumen
- 2click to revealUmbrella cells
- 3click to revealTransitional epithelium
- 4click to revealSmooth muscle (detrusor)
- 5click to revealAdventitia