Striated?
✓ Yes
Voluntary?
✓ Yes
Nucleus position
Peripheral (many)
Cell shape
Long cylinder
Unique feature
Multi-nucleate
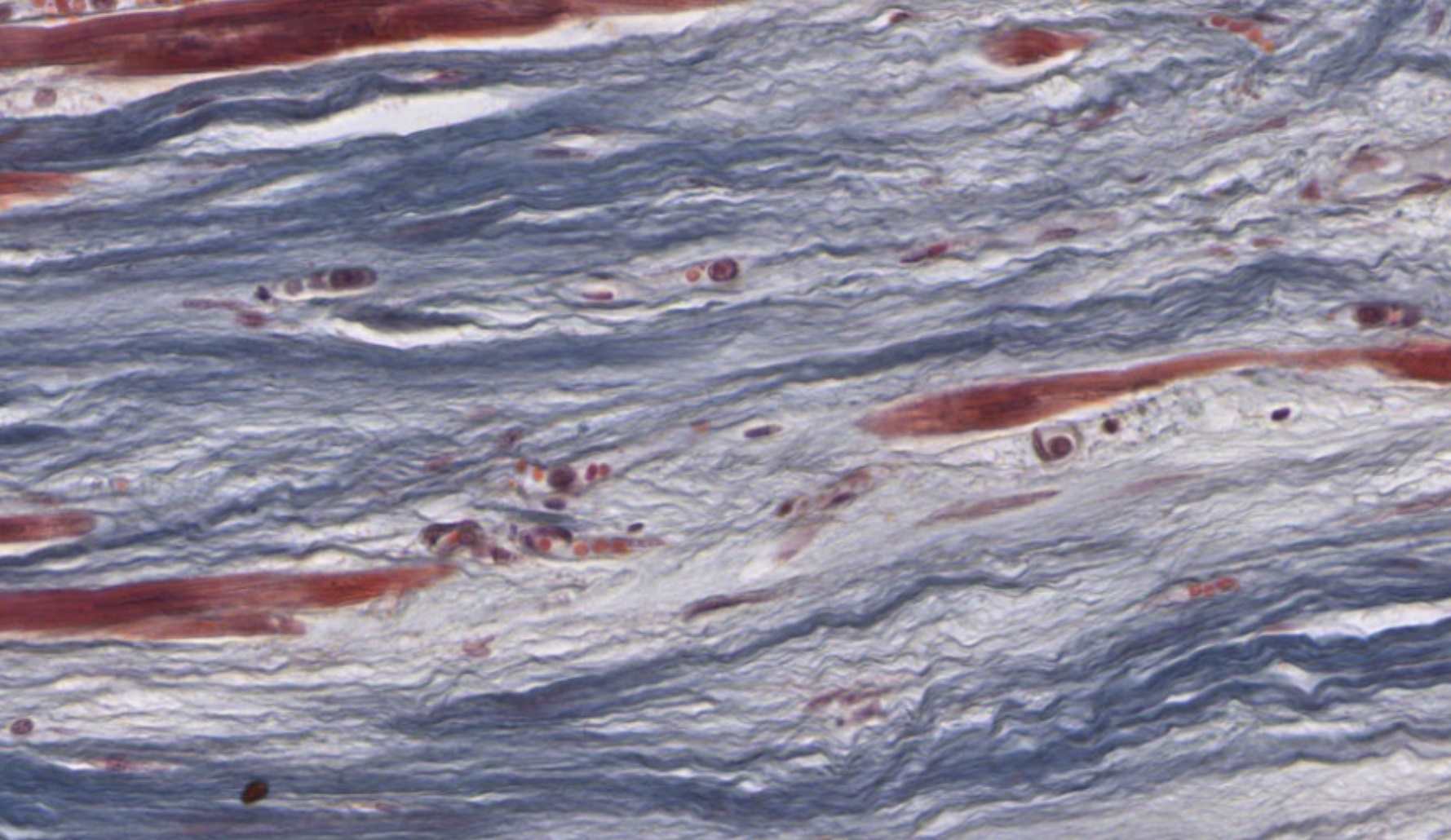
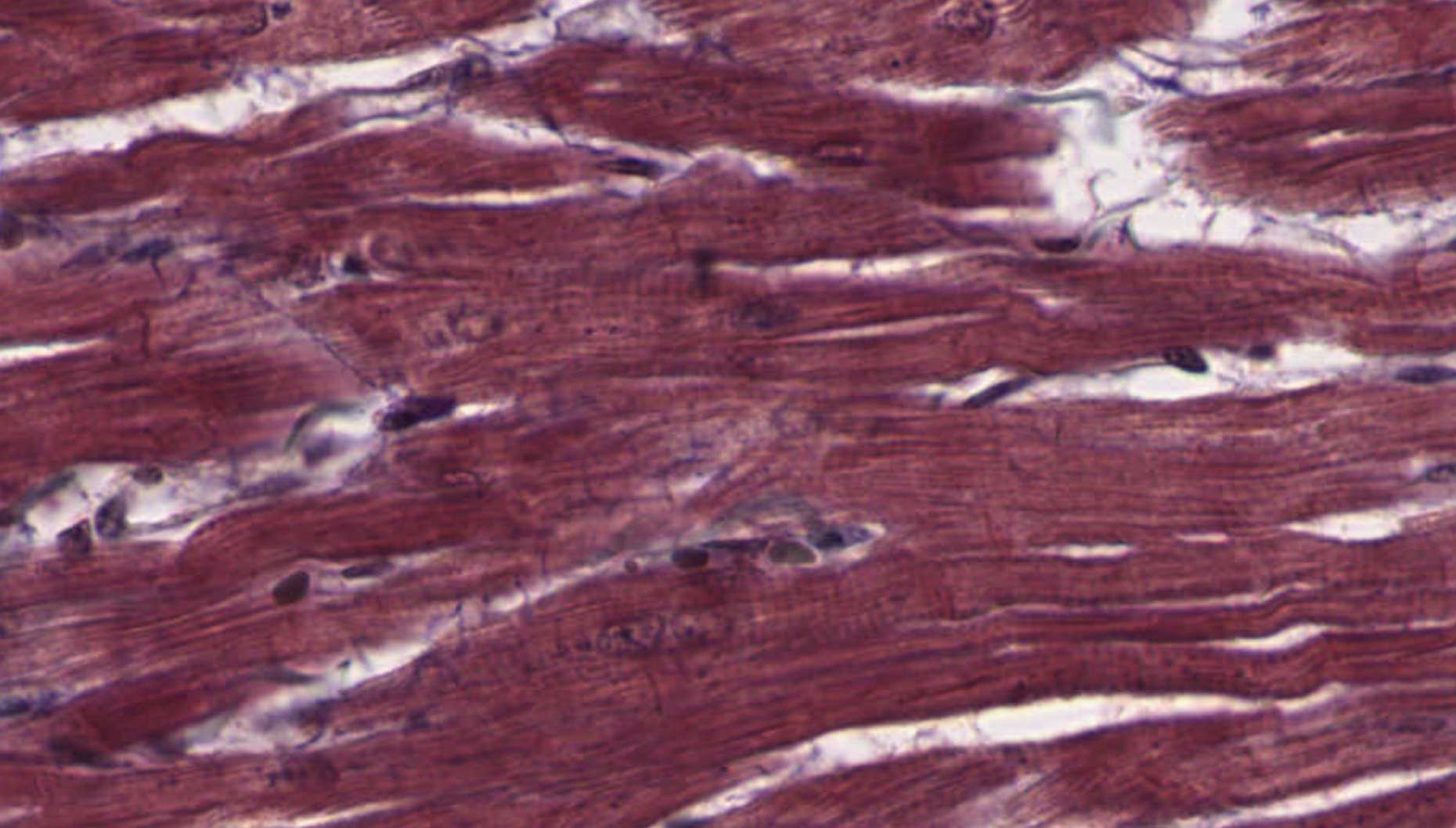
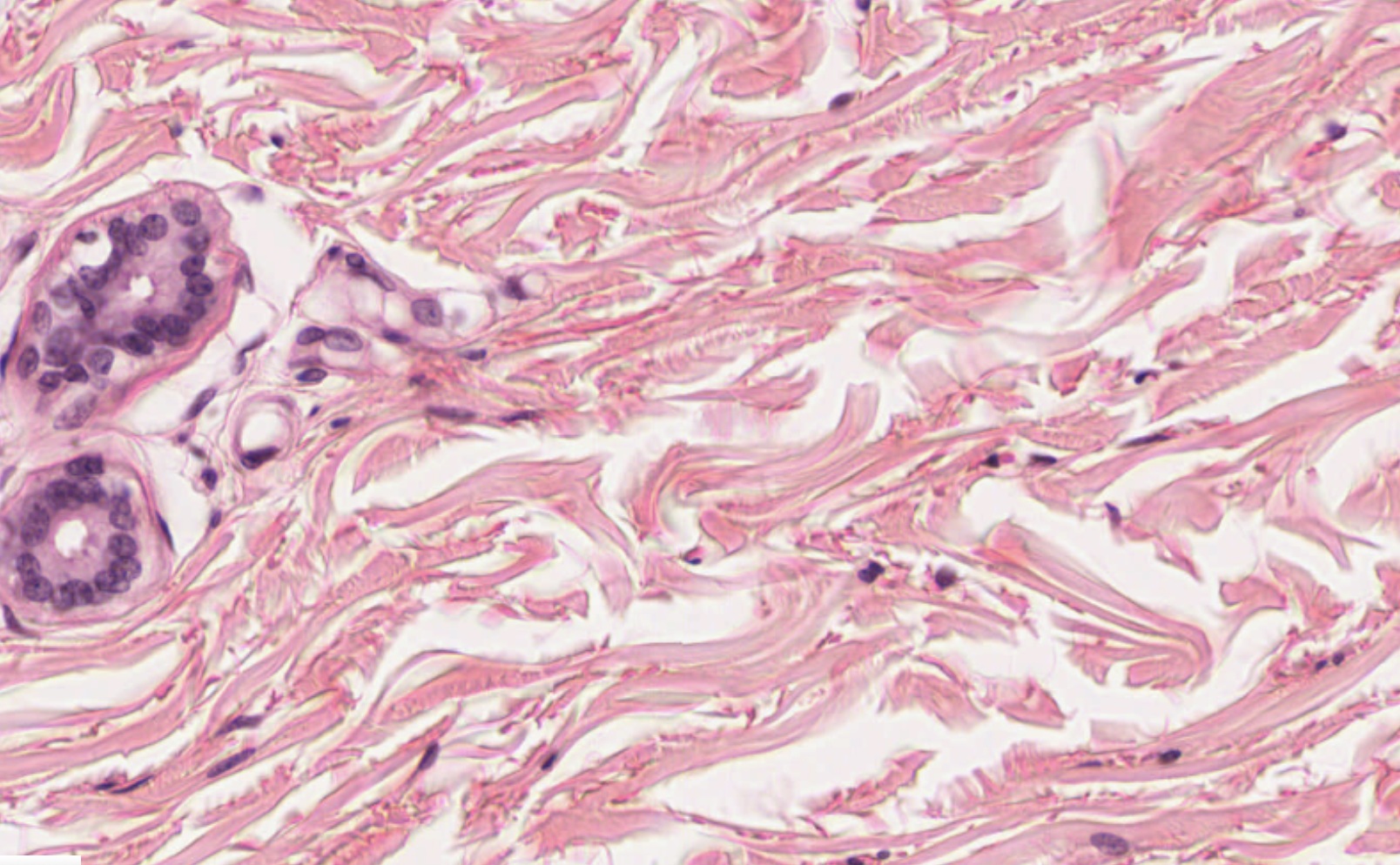
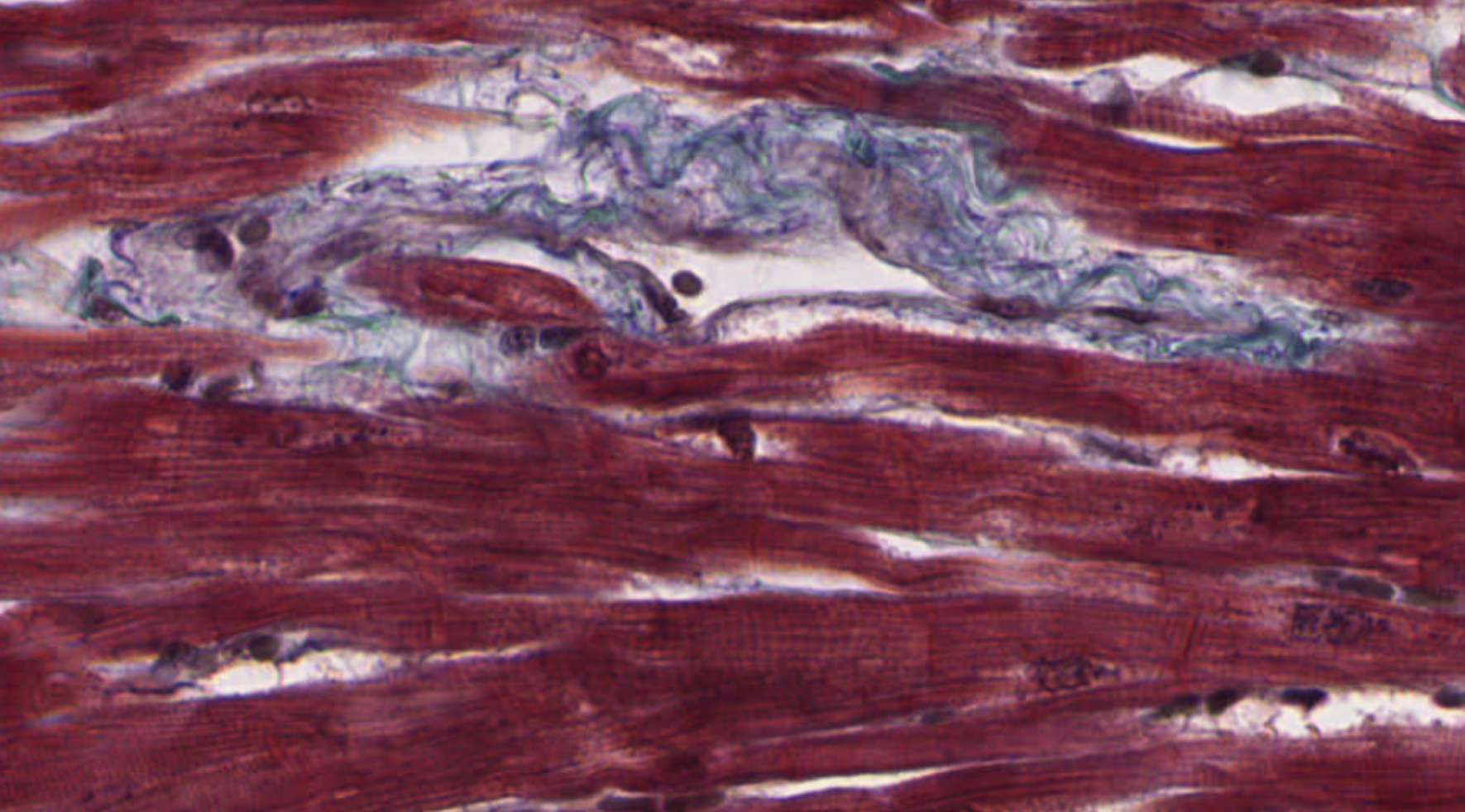
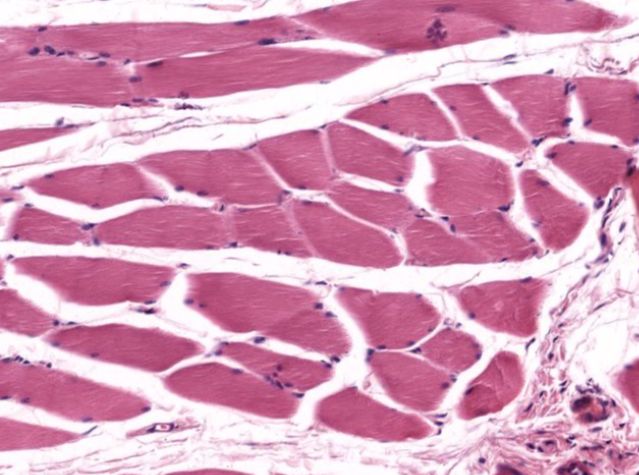
Why two views? A muscle fiber is a long cylinder. Cut it lengthwise → long ribbons with striations visible (longitudinal). Cut it face-on → circular profiles with nuclei at the outer rim (cross-section). Same tissue, completely different image. Histologists always look at both.

Skeletal muscle — longitudinal section · H&E · Slide 058-Thin · University of Michigan Histology (CC BY-NC-SA 3.0)
Click each numbered chip to reveal the labeled structure

Skeletal muscle — cross section · H&E · Slide 058-T · University of Michigan Histology (CC BY-NC-SA 3.0)
Click each numbered chip to reveal the labeled structure
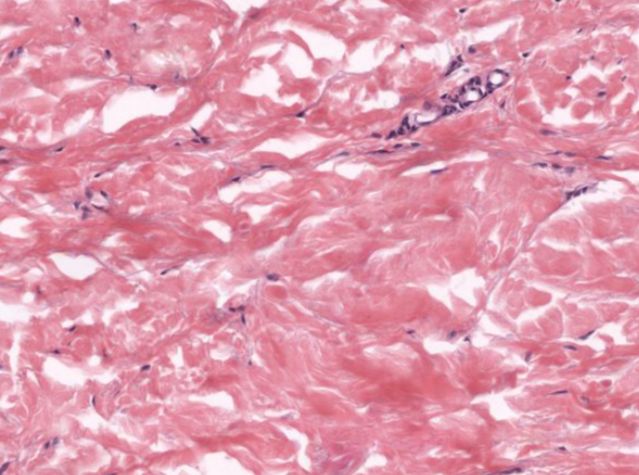
Clinical Connection — Duchenne Muscular Dystrophy (DMD)
DMD results from a mutation in the dystrophin gene. Dystrophin links the sarcolemma to the internal cytoskeleton, stabilizing the membrane during contraction. Without it, the sarcolemma tears repeatedly, calcium floods the cell, and the fiber degenerates. On H&E, affected muscles show fibers of wildly variable size, centrally-relocated nuclei (a regeneration sign), and replacement by fat and CT. The peripheral nucleus you just labeled? Its position is the first thing that changes in a diseased fiber.
⚡ Quick Check — Skeletal Muscle
Skeletal muscle fibers are multinucleate — one fiber, many nuclei. Where do all those nuclei come from?
AnswerEach fiber formed by the fusion of many embryonic cells called myoblasts. All their nuclei remain in the merged cell — hence dozens to hundreds of nuclei per fiber. They're pushed to the periphery to make room for myofibrils, which occupy over 80% of the cell's volume.
In a cross-section, a student points at dots near the centers of fiber circles and calls them nuclei. Are they correct? What's the giveaway?
AnswerNo — skeletal muscle nuclei are peripheral, pushed to the outer edge. Central nuclei indicate cardiac muscle or a regenerating/diseased skeletal fiber. If you see central nuclei in skeletal muscle, that is a diagnostic red flag.